Twenty-Two Years….
The appointment was routine. That was the part I kept coming back to afterward—how completely routine it was supposed to be.
I was in my early thirties, recently married, a new father. My wife was a few months into her second pregnancy. One morning I noticed I was a little short of breath—unusual enough to mention, not unusual enough to worry about. I called my cardiologist. He wasn’t worried either. Probably minor fluid retention. He ordered the standard workup: chest X-ray, EKG, echocardiogram. The kind of thing you do to rule things out.
He came back into the room, sat down, and said, “Well. Your case just became a lot more interesting.”
Left bundle branch block. Reduced ejection fraction—around 25 percent, closer to 25 than 30. No explanation for why. No history that predicted it. Sometimes congestive heart failure happens because it happens, and apparently I was going to be that kind of case.
The Machine
Pharmaceutical treatment was the first attempt. It didn’t work. My cardiologist referred me to an electrophysiologist—a specialist in the heart’s electrical system—who ran a T-wave stress test and initially wasn’t inclined to intervene beyond a recommendation to adjust the medication dosage.
Then he looked at the stress test results more carefully.
He told me he wanted to implant a biventricular pacemaker—a relatively new device at the time, with three leads instead of the standard two. The concept was straightforward if you understood the underlying problem: a left bundle branch block disrupts the timing signal between the heart’s lower chambers. The signal leaves the AV node for the lower chambers, but only one pathway carries it through. It spreads from one ventricle to the other, late and inefficient. Instead of contracting together, the ventricles fall out of sync, wobbling against each other in a way that reduces the heart’s pumping efficiency. The biventricular pacer takes its cue from the heart’s natural pacemaker—the sinoatrial node—and delivers a signal to both lower chambers a fraction of a fraction of a second faster than the malfunctioning pathway can get it there. Resynchronization. The ventricles beat together again, as they’re supposed to.
He would do it on one condition: the device had to be a combination unit—biventricular pacemaker and implantable defibrillator together. The T-wave test results suggested a statistically probable serious cardiac event within five years. He wasn’t going to put hardware in my chest without a backup.
I agreed to the procedure.
There is a thing that happened during the first implant that I feel I should include for the record, because I have never quite lived it down. They gave me a solid dose of anesthesia—enough for a person of normal metabolism. As it turns out, I burn through anesthetic quickly. As they were getting well into the procedure, I apparently decided I had changed my mind and attempted to get up and leave. The electrophysiologist told the anesthesiologist, “Knock his ass out,” which he did. I remember all of this with uncomfortable clarity and we laughed about it afterward, though the EP was perhaps more amused than I was.
A year after the implant, my ejection fraction was back to 55 percent. Normal range. The machine had worked.
The Years That Were
What followed was, for a long stretch, a functional life. Normal, mostly.
I worked—hard, more than I should have, a hundred hours a week some years. I traveled: across the United States, months at a time in Germany, a trip to England. The device required generator replacements every three or four years, each one its own minor ordeal, but mostly uneventful. I later developed type 2 diabetes which I managed through diet and supplements alone, and largely succeeded. I monitored my fluid intake and output, kept an eye on my weight, stayed as active as my condition permitted.
By most measures, I was doing better than I had any right to expect. I knew what was running under the hood. I just chose not to let it be the whole story.
The second generator replacement disabused me of any notion that these procedures were purely routine. Having established at the first implant that I metabolize anesthesia quickly, they gave me more this time. Not quite enough. I came out of sedation just as the electrophysiologist was closing—fully conscious and feeling every pass of the suture needle as he stitched me up. They’d already given me as much as they could safely administer; I lay there and let him finish, which remains one of the stranger experiences I can report from a life that has accumulated several of them.
Around fifteen years in, without warning and without any apparent cause, I began to decline again. Back down to 25–30 percent ejection fraction. The cardiologist at the time was certain it was blockages—plaque, occlusion, the usual culprit. He ordered an angiogram. They went in and found nothing. The plumbing was immaculate. No blockages, no plaque accumulation to speak of. He referred me to a specialist—a heart failure cardiologist—who would manage my care for the years that remained.
They never figured out why the decline happened. They never figured out why the original diagnosis happened, either. Congestive heart failure isn’t always a mystery with an answer waiting to be found. Sometimes it’s just the answer.
What Covid Did
I was out of the workforce by 2016, 2017. I had applied for Social Security disability—my condition and its documented severity were on the agency’s pre-approval list—and was rejected. I hired an attorney and sued. Eighteen months later, I was awarded benefits and a modest amount in back pay, a portion of which went to the attorney. By then, the financial damage was done in ways I haven’t fully recovered from. The ejection fraction by this point had settled around 20 percent, creeping toward 15–20. I added Jardiance to the regimen—not primarily for the diabetes, but because the evidence for its cardiac benefits was becoming difficult to ignore. I held the line.
Then, early 2020: I became ill in a way I had no reference for. Sick enough that I could not breathe. Blood sugar spiked to 390-plus—the highest reading I had ever seen. I passed out.
Covid had not yet been officially identified in the United States, or so we were told at the time. I don’t know what I had. I know it was unlike anything I had experienced in my life before it and it hit my lungs hard.
After about a week, it passed. A month later, I was taking a nap when my pacemaker fired.
I didn’t know that part until later. What I knew was that I woke up and someone was pounding on the front door. I went downstairs and found paramedics on the porch. They walked me out to the ambulance and put me on the monitors. While I had been unconscious, my heart had gone to 360 beats per minute—a catastrophic supraventricular tachycardia. The device had fired and reset the rhythm. I had been entirely unaware of the event. I was now, however, stuck in atrial fibrillation, and the paramedics were suggesting strongly that I go to the hospital.
I was certain it would self-correct. I declined.
Twenty-four hours later, it had not self-corrected, and the cardiologists were considerably less diplomatic in their suggestion. I went. This was the first time I encountered amiodarone—the antiarrhythmic drug they reached for when the rhythm wouldn’t reset on its own. Medication couldn’t stop the AFib. They set a deadline: forty-eight hours, then cardioversion. A few hours before the deadline, my heart reset itself. I went home.
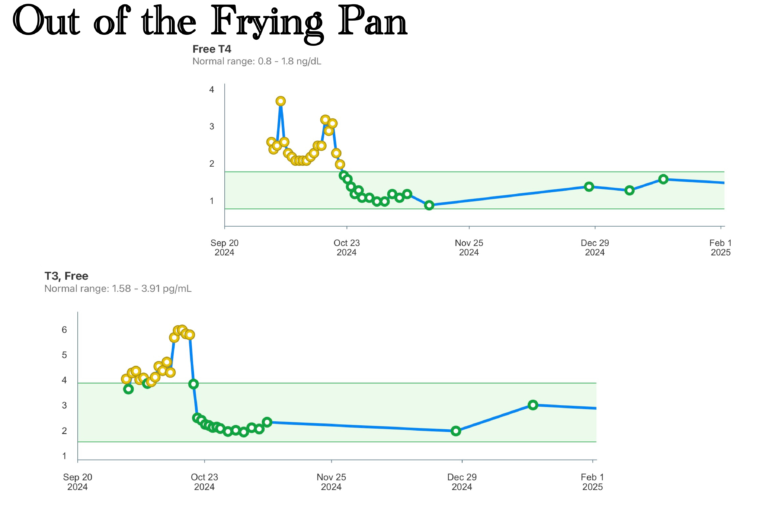
June 2024
Routine bloodwork, routine monitoring. I had been on amiodarone for several years by then—down to 100 milligrams twice daily, but I had never been able to convince my electrophysiologist to take me off it entirely. The thyroid panel came back in June looking acceptable. Cholesterol a little elevated, which was normal for me. Nothing alarming.
Two months later, the atrial fibrillation returned and didn’t stop. Not one episode—sustained, recurring bouts over three weeks. I had managed for twenty-two years with a single hospitalization. I went back.
My ejection fraction was 5 percent. The thyroid hormone levels were through the roof. The amiodarone—the drug that had controlled my rhythm for years—had finally pushed the thyroid past its limit, sending it into a hyperthyroid state that compounded everything else into a crisis that could not be managed at home or managed away.
The second hospital stay of my life began. It would not end the way any of the others had.
Five percent. Routine.
Discover more from One More Beat
Subscribe to get the latest posts sent to your email.



Whoa. This is a heck of a tale. I’m buckled up and awaiting the next installment.
Chag sameach to you & yours.