The House Before the Door Opens
The discharge date arrives and the caregiver shifts into a different kind of motion. The vigil is ending. The person they love is coming home. After weeks of waiting and managing and absorbing things that had no resolution, there is finally something concrete and completable to do.
So they clean the house. They move furniture. They make lists. They prepare.
What they are preparing for, most of them, is the person who left. That is the first problem.
The House Is Not Clean Enough
What “clean” means for an immunosuppressed transplant recipient is not what clean means in ordinary life. The distinction matters enormously, and almost nobody explains it before discharge.
A transplant recipient in the early post-surgical months is operating without the immune defenses that protect most people from ordinary environmental exposure. Bacteria and fungi that a healthy immune system processes without incident become genuine threats. This is not anxiety. It is biology, and the home environment has to reflect it.
Clinical-standard cleaning is not the same as visually clean surfaces. High-touch areas—door handles, light switches, countertops, bathroom fixtures—need to be treated as transmission vectors, not just wiped down. The cleaning products matter. Products that make surfaces look clean and those that actually reduce microbial load are not the same, and the distinction is not academic.
Air quality is part of this. HEPA filtration is not a luxury, not optional. The transplant team will specify; the caregiver needs to have it running before the patient arrives, not purchased the week after. One friend had his air cleaner running in his bedroom before the patient came home. The patient’s mother had hand sanitizer mounted and ready in every room. These were not overcautious gestures. They were the correct response to documented medical need.
The caregiver who does this work is not being neurotic. They are doing what the medical team assumes someone is doing—without always making that assumption explicit.
The Physical Environment
The patient coming home from a heart transplant is not the patient who left for the hospital. They have had their sternum sawed open, wired shut, and left to begin the long process of healing. They are operating under sternal precautions that will govern every physical interaction with the environment for weeks—and the house needs to reflect those precautions before they walk through the door.
The specifics: nothing over ten pounds. No pushing or pulling. No reaching overhead. No twisting. These are not preferences or suggestions. They are the mechanical limits within which a healing sternum can do its work without risking non-union or structural complication. A sternum that is asked to do too much too soon does not necessarily announce the damage immediately. It just heals wrong.
The house has to be arranged around those limits. Not after the patient has already reached for something on a high shelf and felt the pull. Before.
Frequently used items moved to accessible heights. Pathways cleared. A sleeping arrangement that minimizes stair navigation in the first days if stairs are a problem. A shower chair—because standing for a full shower is too much in the early weeks, and because hot water drops blood pressure in ways that create fall risk. Grab bars if they aren’t already there. Non-slip surfaces in the bathroom.
The shower chair is worth naming specifically because it is the item most caregivers don’t think of until the first shower attempt. The transplant team includes it on most discharge checklists without fully explaining why. One caregiver had a shower chair in storage from her own past hospitalization and had it ready before the patient came home. That is the exception. Most people figure it out the hard way.
The caregiver who walks through the house with sternal precautions in mind before discharge will find things to move in every room. The one who doesn’t will watch the patient encounter them repeatedly—each time a quiet reminder that the house was built for the person who used to live there.
The Medication Infrastructure
The discharge paperwork will include a medication list. What it will not include is a system for managing that list over the weeks and months ahead.
The transplant medication schedule is not complex in the way that requires medical expertise. It is complex in the way that requires organizational infrastructure—multiple medications taken at specific times, some with food and some without, some requiring a consistent interval from other medications, all requiring documentation. Tacrolimus levels in the blood are measured from trough samples, drawn just before the next scheduled dose. The timing of doses has to be consistent enough that those labs can be interpreted meaningfully. A pill taken two hours late on biopsy morning produces a misleading result.
A pill organizer system, labeled by day and time slot, reduces that kind of error. It is not glamorous. It is essential.
The daily vitals log is the other piece. Weight, temperature, blood pressure, heart rate, blood glucose if applicable—documented at specified intervals, available for review at every clinic visit. The transplant team uses this data to track trends and catch early warning signs. They are relying on whoever is managing the home environment to generate it accurately and consistently.
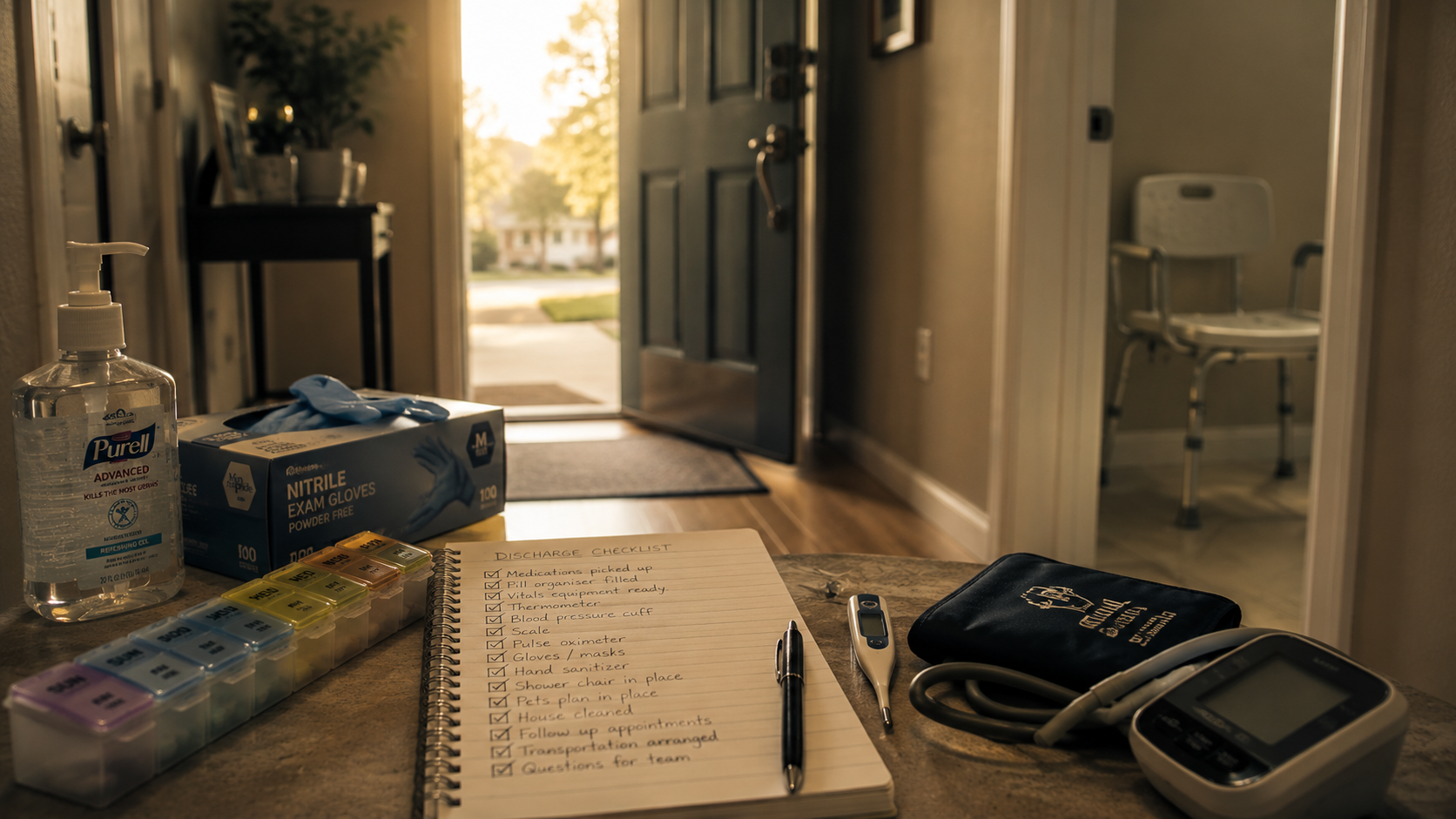
The equipment for all of this should be in place before the patient arrives home: calibrated scale, digital thermometer with disposable covers, blood pressure cuff in the correct cuff size, pulse oximeter. These are not expensive. They are not optional. They are the instruments of a monitoring system that the transplant team assumes is already running.
The Food
What needs to be in the house and what cannot be there are two different lists. Both matter. The second one is more urgent.
Grapefruit and pomegranate—and their juices—need to be out of the house before the patient arrives. Not set aside. Out. Both inhibit the CYP3A4 enzyme pathway that metabolizes tacrolimus and sirolimus, the primary immunosuppressants. Consuming either raises drug levels unpredictably, potentially into toxic range. This is not a dietary preference or a loose precaution. It is a pharmacological interaction with documented clinical consequences, and it applies every time, not just when levels seem borderline.
Star fruit, soursop, and certain herbal supplements including St. John’s Wort carry similar concerns. The transplant team will provide the specific list. The caregiver’s job is to apply it to what is currently in the kitchen—not after the patient is home and the question comes up, but before.
The positive list is more complicated because it shifts. Early post-transplant, dietary restrictions for an immunosuppressed patient include avoiding raw or undercooked proteins, unpasteurized products, and certain high-risk fresh produce. Food safety practices that are relaxed in ordinary life become clinically relevant. The transplant team’s nutritional guidelines are the authority here.
Then there is prednisone.
High-dose prednisone in the weeks immediately following transplant produces appetite and taste disruption that most caregivers are not warned about in sufficient detail. Voracious hunger is common—not ordinary appetite, but an escalating physical demand for food that can be difficult to satisfy within dietary constraints. Taste disturbance is also common: foods that the patient talked about wanting throughout the hospitalization may taste wrong, flat, or simply unappealing when they arrive home.
The caregiver who stocked the kitchen with the patient’s favorites—the things they missed, the meals they described wanting during the long weeks of hospital food—may find that none of it lands the way anyone expected. The patient who has been dreaming about a specific meal for two months may sit down in front of it and feel nothing.
Stock for flexibility. Stock for easy preparation. Stock for a reality that will shift faster than anyone can plan for, and that has very little to do with what the patient wanted before any of this happened.
Pets and People
Two separate problems that share the same underlying question: who—or what—in this household represents an infection risk, and what is the plan?
Pets first. The dog or cat that has been sleeping in the bed, sitting on the furniture, licking hands—this animal is a source of zoonotic bacteria and fungi that the transplant team takes seriously. This does not mean the patient can never be near their pet again. It means that in the early post-transplant months, when immunosuppression is at its most aggressive, certain exposures require management. Litter boxes need someone else to handle them. Animal dander and waste carry organisms that healthy immune systems clear routinely and compromised ones cannot. The transplant team will give specific guidance. The caregiver needs to have acted on that guidance before the patient comes home, not after the first incident.
If there is no plan for the pet, a plan needs to exist. Not “we’ll figure it out when he gets here.” An actual plan, in place, operational on day one.
People next. Anyone in the household who is sick—cold, flu, stomach virus, anything respiratory—is a reason to delay discharge or make alternative arrangements. A transplant recipient cannot come home to a household with illness circulating. A transplant recipient exposed to household illness in those early weeks may find themselves back in the hospital, undoing hard-won progress before recovery has had a chance to begin.
The plan for sick household members needs to exist before the door opens. If the caregiver is the one who gets sick, there needs to be a backup. The transplant team assumes there is a backup. Whether there actually is one depends entirely on whether someone has thought it through in advance.
The Items Nobody Thinks Of
Not on any official checklist. Figured out the hard way.
Adhesive remover wipes, for the surgical tape and dressing adhesive that leaves residue on skin that ordinary washing doesn’t reach. Nitrile gloves for dressing changes and any wound care. Masks—not one box but a supply—because household members will be masking around the patient in the early months whenever there is any illness question at all. Comfortable loose-fitting clothing that does not require overhead reaching or tight waistbands across a healing incision.
Easy meals that can be heated in minutes, because the patient’s energy will be unpredictable and the caregiver will have no margin.
A way to communicate between rooms that doesn’t require the patient to shout. Shouting strains the sternum. Projecting voice may be impossible if there were intubation complications or vocal cord involvement—a paralyzed vocal cord is not uncommon after extended intubation, and it can persist for months. A bell. A text thread with household members. Something low-effort that doesn’t require the patient to compensate physically for a house that wasn’t designed for this.
None of these require medical expertise to source. They require someone thinking ahead, before the first week at home makes thinking ahead impossible.
What Cannot Be Made Ready
The house can be made ready. It takes work—real work, sustained attention, a willingness to walk through every room with new eyes—but it can be done. The surfaces can be sanitized. The furniture can be moved. The pill organizer can be filled and labeled. The forbidden foods can be removed. The shower chair can be in place before the first morning home.
The person coming through that door is another matter.
The patient who left for the hospital and the patient returning are not the same person, and no checklist accounts for that. The medications produce effects that arrive without warning and without proportion to anything the caregiver did or didn’t do. The body that walks through that door has been through something that the caregiver witnessed from the outside but did not experience from the inside. The cognitive and emotional terrain has shifted in ways that neither person can yet fully see, in directions that neither person chose.
The caregiver who has done everything right—who has cleaned to clinical standards, moved the furniture, filled the organizer, stocked the kitchen, managed the pets, sourced the items—will still stand at the threshold when the patient arrives and discover that the hardest part of this transition has nothing to do with any of it.
The house was the part they could control. The rest of this is something else.
Do the work. Source the items. Read the discharge instructions twice. Call the transplant coordinator with the questions that feel too small to ask. Prepare the house as if the preparation matters—because it does.
And then understand that all of that was the easy part.
Discover more from One More Beat
Subscribe to get the latest posts sent to your email.



