
Post Op / ICU
The first few days after a heart transplant are not straightforward.
The body is recovering from major trauma while a new chemical environment is being forced into place, and the two don’t always agree. Signals cross. Responses don’t match their causes. What feels like one kind of problem can turn out to be something else entirely.
This matters, because in those first days, you don’t always know which is which.
Terror Stricken
The morning after the surgery, I woke up in terror.
Not the waking-up-disoriented kind. Not the where-am-I kind. I was fully aware—knew exactly where I was, knew what had happened, knew the surgery was done and the heart was in and everything had gone by the book. My mind was working. My intellect was online.
And I was experiencing the most extreme, abject terror of my entire life.
I did what I always do under pressure: I analyzed. Methodical, immediate, automatic. Run the inventory. Pain? Manageable—nothing beyond what the situation called for. The heart? Felt fine. The room? Stable. The data said nothing was wrong. Nothing in my environment justified what I was feeling. The terror had no object. It was simply there, at maximum volume, with no rational basis whatsoever.
Which told me exactly what it was: irrational. And if it was irrational, I could refuse to let it take over.
I hit the call button. I told the nurse, as calmly as I could manage, what was happening. The team huddled. Someone made a decision.
They dropped the epinephrine.
Almost immediately, the sensation abated. The chemistry retreated. The room came back into proportion.
That was the epinephrine drip—a vasopressor running through my lines to support blood pressure in the immediate post-operative period. A known side effect: acute anxiety, panic, the physiological sensation of terror indistinguishable from the real thing. My intellect had not failed me. It had done precisely what it was built to do—assessed the situation, found no rational basis for the response, and held the line. What would have overwhelmed most people was, for me, a problem.
Later, when they pulled the epinephrine line, a small amount of residual medication trickled through the connector before it cleared. The terror rose again—brief, sharp, unmistakable. This time I already knew what it was. I breathed through it and let it pass.
Chemistry, not psychology. Still—a reminder of how thin the line can be.
The Room
The ICU after a heart transplant does not look like what you picture when you think of a hospital room.

First Morning Post-Op; IVs Consolidated, Already Sitting Up.
There were somewhere in the neighborhood of a dozen IV machines—a wall of them, stacked and humming, each one managing something specific: pressors, fluids, immunosuppressants, pain management, the nitroglycerin drip, a dozen other things I was tracking with varying degrees of clarity. Lines went in and out of me from what felt like every direction. The monitors ran constantly. The room never fully quieted.
Among the lines was an external pacemaker—wires running directly into my chest, there as a precaution while the new heart established its own rhythm. When the time came to remove them, the process was exactly what it sounds like: pull them out a little, snip, let them retract back into the body. They stay in there. Something worth knowing, if not worth dwelling on.
My vision was wrong for the first two days. Not blurred exactly—more like the signal wasn’t quite resolving. I couldn’t read, couldn’t type, couldn’t manage a phone. My first texts went out by dictation, a nurse helping me get the words right. The first post-op update to the wall—the one that went out under Teresa and Mom’s names on November 10th—was theirs, not mine. I was still finding my way back.
On the morning of November 11th, I texted my mother: I don’t even know how to breathe yet.
She said: it’s only day two.
She was right. But from inside it, day two felt like its own kind of eternity.
The New Heart
At some point in those first days, someone told me my ejection fraction.
Going in: 5–10%. On the Impella, headed for an RVAD, a heart that was failing at its most basic function.
Coming out: 58–63%.
I had known, intellectually, that a transplant would produce a significant improvement. I had read the literature. I understood the numbers. What I had not understood—could not have understood without experiencing it—was what that improvement actually felt like from the inside. The strength in the chest was already there when I woke up from surgery, the evening of November 9th. It had been there before I had words for it. The new heart was doing its job with a force and consistency my native heart had not managed in years. Possibly longer than I could accurately say.
The number confirmed what I had already felt.
Moving
By November 11th—day two—I was up and walking the hallways.
This is the protocol. The piece on waiting explained why: immobility destroys muscle, compromises pulmonary function, increases clotting risk. What that piece described from the outside, this one describes from the inside. The difference between watching ECMO patients walk the ward during the wait and being the patient walking the ward the day after surgery.
PT and OT worked through the milestones in sequence: sitting up, standing, hallway laps, stairs, car transfers—the specific movements a person needs to navigate the world outside a hospital bed. Each one is both functional and symbolic. When you can get yourself in and out of a car, you can go home.
The pace of it astonished people around me. It astonished me too, though less so—I had watched the protocol work from the other side of it, and I understood what it was designed to do.
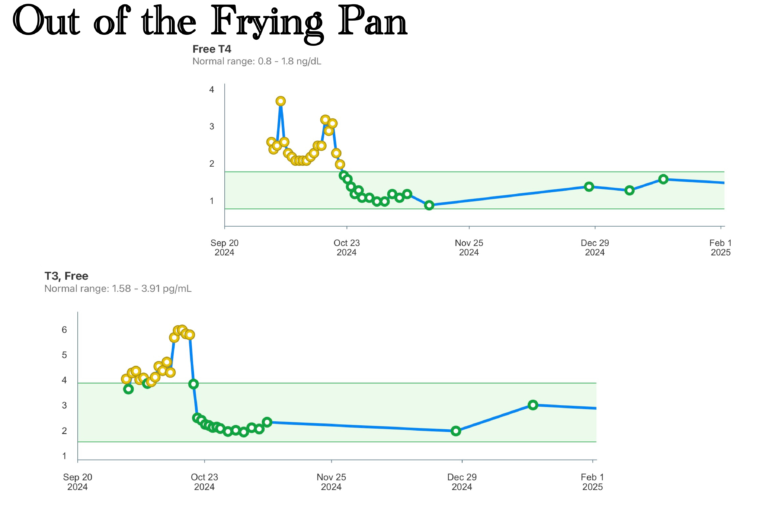
The ICU Problems
The nitroglycerin drip produced headaches. This is documented, known, a listed side effect.
The night shift, when I raised it, did not act on it.
The day shift noted it immediately.
Dowling came through and dialed the drip back by fifty percent. The headaches resolved.
The move to the step-down unit came on November 14th. I was ready to leave the recovery ICU behind in every sense—the night shift, the noise, the particular quality of inattention that had let a documented side effect go unaddressed through the hours when it mattered most. Step-down meant progress. It also meant escape.
Taste
Somewhere in those first days, I noticed the food was wrong.
Not wrong in the way hospital food is usually wrong. Wrong in a more fundamental way—flat, muted, arriving without the information food is supposed to carry. The prednisone was doing what prednisone does: suppressing the immune system, managing inflammation, and in the process stripping the taste receptors of their sensitivity. Everything tasted like a diminished version of itself.
In the hospital, this was tolerable. The food was not good to begin with. A baseline of institutional mediocrity is not hard to fall below when your palate has been chemically neutralized.
Coming home would be different. That story belongs in the next piece.
The Chest Drainage
I went home on November 18th with one drain still in—a collection ball attached to a tube coming out of my chest, there to manage residual fluid from the surgical site. This is not how it is supposed to go. It is, however, sometimes how it goes.
The first day home was extraordinary. My own bed. My own bathroom. Vox Machina on the television, season three, watched straight through. The world outside the hospital existing again.
The second day, the fluid changed color.
I was readmitted on November 20th. The working hypothesis was infection—the thing that, in a newly transplanted, immunosuppressed patient, carries the most serious implications. I had been warned. Everyone had been warned. A possible infection means immediate attention and the possibility of days or weeks of treatment.
The picture clarified overnight.
Not infection. A nicked lymph node—a small complication from the surgery, leaking chyle into the chest cavity. The evidence: high triglycerides in the drainage fluid. The treatment: an ultra-low fat diet, sustained for several weeks, to allow the lymph node to seal itself.
I was home again on November 21st. One night.
The diet prescription deserves a moment of acknowledgment for the specific cruelty it represented. I am diabetic. The standard management approach for diabetes is to reduce carbohydrate intake and replace those calories with fat—healthy fats, but fat. Ultra-low fat and diabetic management are in direct, structural conflict. The two requirements do not coexist gracefully. I worked through it. There was not another option.
The Lights
On November 16th—one week out—I posted to the wall:
I had absolutely no idea just how diminished a capacity I’ve been operating at. What’s more, I had no idea just how long I’ve been operating in such diminished capacities.
The cognitive return had been underway since the Impella. The new heart accelerated it. What had been a gradual brightening became something faster and more definitive—the lights coming back on in rooms that had been dark for years. The intellectual machinery running at a speed I had stopped expecting.
I had operated at diminished capacity for so long that diminished had become normal. The return of full capacity did not feel like recovery. It felt like something being restored that I had almost forgotten I once had.
A New Baseline
Two weeks out. EF 58–63%. Sleeping in my own bed without beeps or interruptions for eight hours straight.
I wrote to the support group:
2 months in the hospital was brutal—the constant pain of the process with needles, tubes, scalpels, and lines was more than just unpleasant. The early uncertainty then the wait was excruciating. Every button, fear, and emotion pushed to the limits. The end result, though—I am alive, with my loved ones, and there is a future.
Now THAT, friends, is pretty dang cool.
Discover more from One More Beat
Subscribe to get the latest posts sent to your email.



Profoundly cool, yes. 🙂