The Waiting
Tom Petty said it as well as anyone ever has. The waiting really is the hardest part—but not for the reasons most people assume. It isn’t a matter of patience. Patience implies something you can summon—a discipline you can practice. This is something else entirely.
The runway is short, and the solution to a successful lift-off isn’t yours to control. It’s a matter of nature and design—of biology and timing and a stranger somewhere whose story you will never fully know. You’ve done what you can do. The pre-tests are finished, the decline is slowed, the machinery of medicine has been set in motion. And then life continues without you.
That disconnection—being set aside while the world moves on—is expected. Normal, even. The staff will tell you so. That doesn’t make it easier to accept.
So you wait. You wait for the next shoe to drop. You wait for the heart to find its way to you. You wait for the next day to arrive, because the next day is all you’ve got even though it is not guaranteed.
One minute, one hour, one day becomes a few days. Becomes a week. Becomes a month.
And it is brutal.
How the List Works
Status 2 is not the bottom of the transplant list, but it is not the top either. Above me were patients on ECMO—extracorporeal membrane oxygenation, a machine that takes over for both the heart and the lungs simultaneously. Below me were patients stable enough to wait at home. I was in the middle: sick enough to require the Impella running continuously, not yet sick enough to qualify for the highest urgency status. As long as the Impella was running, I was Status 2. That was the ceiling and the floor at the same time.
Every two weeks at Status 2, the clock expires. The transplant team files an extension request—a formal case to UNOS arguing that the patient still qualifies, still needs the heart, still deserves the spot. It is not automatically approved. The one condition that reliably killed a relisting, the nurses told me, was infection. Short of that, the team made their case and the case was generally made. One patient, they mentioned, had been relisted three times. More than two months of waiting, of two-week clocks, of extensions filed and approved and filed again.
I was trying not to think about that.
The Texture of It
There is a specific quality to hospital boredom that has no civilian equivalent. It is not the boredom of a slow afternoon or a long flight. It is boredom layered over something closer to suspended animation. You cannot fully relax because the next thing is always coming. You cannot fully engage because you are attached to machines and the cognitive overhead of being a patient is relentless.
And the next thing is always coming because the hospital never stops.
The parade begins around 4am. Radiology arrives first, usually, for the morning chest X-ray. Then phlebotomy. Then the EKG tech. Then the first physician of the day, then the second, then the residents trailing behind them. Food service. Supply restocking. The nurse’s medication rounds. By mid-morning you have already been awake for hours and interacted with a dozen people and the day has barely started. It runs straight through to 10pm, with overnight checks every hour or two beyond that. Even the “sleep holiday”—a formal designation where the staff is supposed to grant you an uninterrupted block of five or six hours—produced interruptions. The sleep holiday was aspirational. You do not rest in a hospital. You endure it.
Which is why the walking mattered.
The standing order for transplant patients is to keep moving, and the reason is not mysterious: immobility destroys muscle at a rate most people do not appreciate. Days in bed produce measurable atrophy, compromise pulmonary function, and increase clotting risk. The psyche takes its own damage from horizontal confinement. The antidote is laps—three laps of the ward, roughly a third of a mile, more when my body cooperated. Some days it did. The Impella had been dialed back slightly to ease the toll on my platelets ahead of surgery. That adjustment reduced both my support and my stamina, so I went as far as I could and stopped when the heart rate climbed too high.
I was not the most determined walker on that floor. ECMO patients were up and moving the ward. If you do not know what ECMO is, look it up—and then consider what it means that people on full cardiopulmonary bypass were doing laps. That really says something. The protocol exists for a reason, and the patients who understood that were the ones who gave themselves the best chance.
I watched everything. I finished The Rings of Power and was furious at where they ended the season. I worked my way through The Chosen and started recommending it to Niles, who was skeptical and then wasn’t. Niles, for his part, sent me a ham radio study manual—his solution to the problem of my restlessness was to give me a license to pursue. I was going to study for my Technician certification from the hospital bed. I never opened it. The intention was enough.
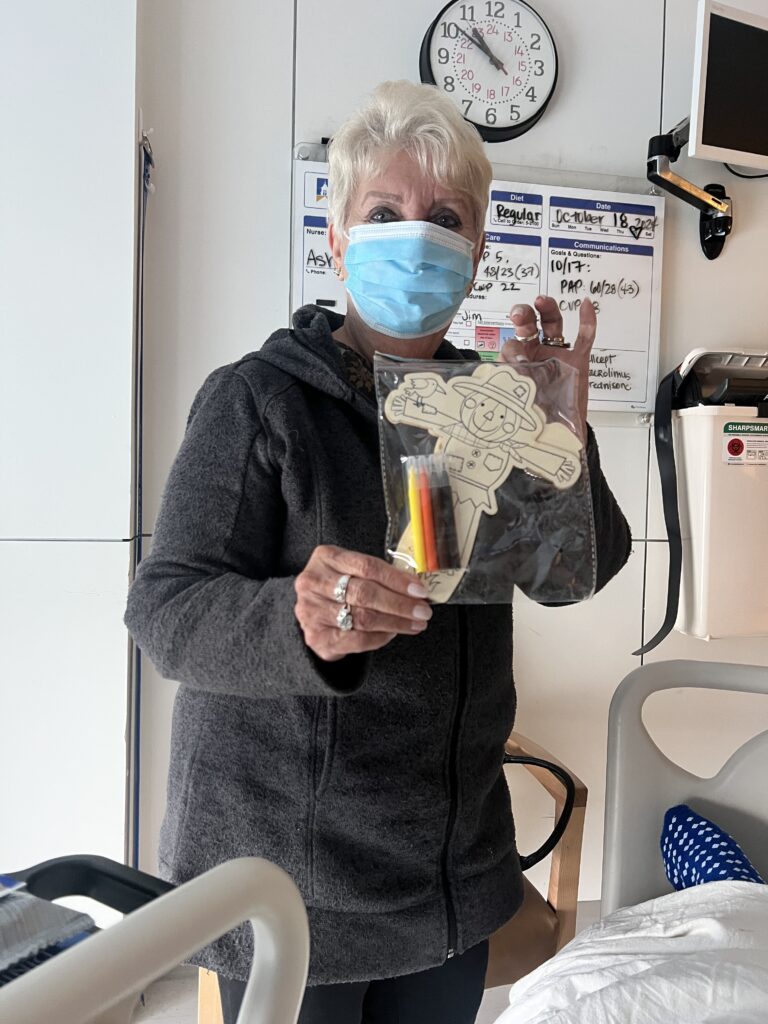
Mom brought a Smokey Bear paint-by-number kit and some coloring books. She and Lisa had assembled a small arsenal of notebooks, pencils, crayons. The instinct was right even if the execution was optimistic—I was not, at that particular moment, a coloring book person. But the kit sat on the windowsill and made me smile every time I looked at it, which was probably the point.
On a rainy Friday when Niles couldn’t make the drive, I put on Bob Marley and told him to go clean his kitchen instead. He sent me progress photos. It was funnier than it sounds.
Music Fills the Gaps
Music filled the gaps.
Not as distraction—as structure. Something to measure the hours against. The days had no natural boundaries. The nights were worse. Sleep came in fragments, if it came at all. The monitors, the checks, the noise of the ward—it doesn’t stop.
Music gave the time somewhere to go.
Bob Marley ran for stretches. There is a steadiness in that music—a perspective that does not rush, does not panic, does not collapse under pressure. It carries a kind of internal alignment that translates, if you let it. It helped hold the line.
Tom Petty came back through as well. The waiting is the hardest part. That line lands differently when you are actually doing it—when the waiting has weight and consequence and no defined endpoint. It stops being a lyric and becomes a description.
At night, I used what I can only describe as spa music. Simple, repetitive, ambient. Not something I would have listened to under normal circumstances. In that room, it became essential. It gave me something to focus on when the pain was up, when the body wouldn’t settle, when sleep was possible but not yet accessible. It became a form of meditation—something to follow instead of the noise, instead of the discomfort, instead of the clock.
And then there was the Billy Joel moment.
I closed the door and tried to sing. What came out was not a voice. One cord working, one not. A growl where something else should have been.
That was the only time I broke.
I said it out loud, to no one in particular: Whatever you do, don’t take my voice. I can die, but I cannot lose the gift of song. The cost is too high.
A few tears…a moment. That was it.
Then it passed. Like everything else in that room, it passed.
Music went back to being what it had been from the start: a way to hold the line.
The Potassium Battle
The most frustrating sustained thread of those weeks was not the AFib, not the procedures, not the sleeplessness. It was potassium.
The connection was not subtle. When my potassium dropped below a certain threshold, AFib followed with an eerie, almost mechanical predictability. Every single time. The solution was straightforward: keep the potassium up. The execution was, inexplicably, a sustained fight.
The ICU runs on protocols. NPs manage the floor, physicians sign off, and the playbook covers most patients most of the time. I was not most patients most of the time. I needed more potassium than the sliding scale provided, and getting the scale adjusted required a level of advocacy that was exhausting on top of everything else. They won’t listen and they can’t seem to do the math—that was my assessment in the moment, and I stand by the frustration even if the framing was uncharitable.
I want to be clear: the staff at The Christ Hospital provided genuinely outstanding care throughout an extraordinarily complicated hospitalization. This was one friction point among weeks of exceptional attention. I note it here because recipients and caregivers in similar situations deserve to know that self-advocacy on something this specific and this consequential is sometimes necessary—and is always worth it.
A Crack in the Armor
There was one moment where I lost it.
Not dramatically. I did not throw anything or raise my voice. I became short—clipped, impatient, unpleasant in the exact way prolonged exhaustion produces. It came out sideways at a nurse over the potassium. It was the only time in the entire hospitalization that the seams showed.
The context matters, though it does not excuse it. By late October I had been inpatient for nearly a month. I had been through the Impella surgery, the AFib cascade, the cardioversion while conscious, the thyroidectomy, the vocal cord paralysis, the hormonal crash, the swan catheters, the 4am wake-ups, and the grinding, relentless waiting. I was also on high-dose prednisone—40, 60, 80 milligrams—a corticosteroid that at those levels is well documented to produce irritability, emotional lability, and mood dysregulation. I was not simply tired. My neurochemistry was actively working against me.
None of that makes it right. I apologized.
What I remember most is what came after. The nurse put her hand on my shoulder—a quiet signal, the kind that says it’s going to be all right. Something in me released. I dropped my head to her shoulder for a moment and let it pass through me—the weeks, the anger, the frustration, the accumulated weight of all of it. She did not take it personally. She understood completely. That small grace, offered without drama, cost her nothing and meant everything.
I held my composure through things that would have broken most people. I used humor as a pressure valve, intelligence as a sorting mechanism, sheer will to keep moving through a process that was medieval in its demands. The crack lasted thirty seconds. I am not proud of it, but I am no longer ashamed of it either. The staff met it exactly as they should have—and exactly as I should have expected from people who had been doing that for me all along.
October 26th
A heart became available.
The doctor mentioned it during rounds—matter-of-fact, the way they deliver most news up there. A donor heart had become available overnight. It was too small; my BMI put it out of range. They passed.
He said this was encouraging. It meant I was being seen, that the matching process was working, that offers were coming, that I was moving up.
That evening I told Niles I still felt like a heart was coming. Not hope exactly—hope has a fragile quality, a please-let-this-be-true. This was something more settled. A certainty without evidence, which is either faith or delusion depending on how things turn out.
Things turned out.
The Fog Lifting
Somewhere in those weeks, I noticed I could think again.
Not all at once. More like a gradual brightening—the cognitive equivalent of eyes adjusting after a long time in a dark room. I had been, for months—perhaps years, if I am honest—functioning at a level I can only describe as closer to average than I am accustomed to. I want to be precise about this, because the observation is easy to misread: this is not a dig at anyone, not a ranking, not condescension. It is a calibration statement about my own instrument. Intelligence is what I rely on most—the way a surgeon relies on fine motor control, the way a musician relies on pitch. When it degrades, I notice. The degradation had been real, and it had been going on long enough that I had begun to normalize it.
The Impella, doing its job, was improving my cardiac output. More blood moving. More oxygen reaching the brain. The fog was lifting.
I was aware of it most sharply in a text exchange with Eric, who had been reading some fiction I’d written years earlier. I told him my hope was that my cognitive abilities would improve significantly with the new heart—that I would finally be able to get back to the work. I was already planning for a future. That alone told me something had shifted.
For what it is worth: I am probably the world’s worst basketball player. Possibly not the absolute worst, but not far from it. We all have the thing we are not built for. The instrument I was built for was coming back online, and I could feel it.
The Extension
The two-week clock expired. The team filed the extension request—a formality, they told me. I was a hard case by any measure; the argument made itself.
Before the approval came back, the call came.
The extension was still working its way through the process when the match arrived. The team waved it off—don’t worry about it, you never lost your spot, you’re still on the list. The machinery was still running when the thing it was built for arrived.The waiting doesn’t end. It just stops.
Discover more from One More Beat
Subscribe to get the latest posts sent to your email.