The Blood is the Life
At some point during my pre-transplant hospitalization, someone counted. Fifty vials of blood, give or take, drawn over the course of the initial workup—roughly 250 milliliters, a full cup of yourself handed over one tiny vacuum-sealed tube at a time, all in a single sitting. The arithmetic of it doesn’t fully register until you’re on the other end. At The Christ Hospital, in the weeks and months after the transplant, blood draws were a near-daily reality—twice weekly in the early going, then weekly, then monthly as the recovery stabilized. The veins in both arms accumulated the particular geography of a patient under close surveillance: the small bruises, the scar tissue at the crook of the elbow, the involuntary flinch.
That cadence is now behind me. Eighteen months out, I go to the lab once every six months.
I want to sit with that for a moment before moving on to what the blood actually tells us, because the psychological weight of that shift is not nothing. Post-transplant care is intrusive by design. It has to be. But there is a cost to being perpetually monitored, perpetually assessed, perpetually reminded that your continued existence is a managed proposition. The six-month window is not just a clinical milestone. It is breathing room. It is, for the first time in a very long while, something approximating normal.
The Body You’re Managing Now
The body I came home with in November 2024 is not the body I had before. That sounds dramatic; it’s actually just accurate. The transplanted heart itself is the obvious difference—a stranger’s heart, beating without a vagal connection to the nervous system it now serves, unable to modulate its rate the way a native heart would. But the pharmacological reality goes deeper than the organ.
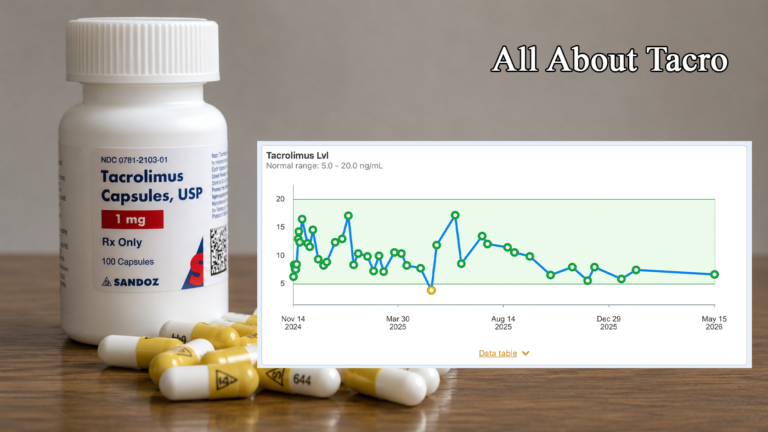
Tacrolimus (Prograf/Envarsus), the primary immunosuppressant, is a calcineurin inhibitor. It keeps the immune system from recognizing the new heart as foreign, which is its job. It also reduces insulin production, which is one of the less-advertised consequences. Sirolimus (Rapamune), the mTOR inhibitor added to my regimen at the one-year mark in response to a CAV diagnosis, dampens insulin sensitivity. Combined, they disrupt the ghrelin-leptin cycle—the hormonal axis governing hunger and satiety—in ways that compound the metabolic damage. This is not, to be very clear, in the direction that helps you lose weight.
The cumulative effect was a body that could no longer manage its own glucose effectively. My A1c climbed. My fasting numbers were higher than they should have been. I was on insulin.
I knew these mechanisms were present because I understood what my medications do. When my bloodwork and continuous glucose monitor data made the picture clear, I went to my endocrinologist and asked specifically about a GLP-1 agonist—Rybelsus, an oral semaglutide—combined with the Jardiance I was already taking. The combination worked. Twenty-five pounds gone in a few months. Fasting glucose averaging 90–100 mg/dL. Insulin discontinued.
The point is not that I made a clever pharmaceutical suggestion. The point is that I could only make it because I understood what I was looking at. That understanding came from the blood.
Three Readers, One Sample
When my lab results come back from the 18-month draw, they will be reviewed by at least three different physicians with three different professional frames: my transplant cardiologists and team, my endocrinologist, and my GP.
Each of them is excellent at what they do. Each sees the whole patient in the clinical sense—they are not tunnel-visioned specialists who ignore everything outside their domain. But each also carries a panel of dozens—probably hundreds—of patients. They cannot live inside any individual case the way the patient does.
I have one patient. I have unlimited time to pay attention to that patient. That is not a criticism of my medical team. It is a structural reality, and it is precisely why the informed patient argument matters.
My transplant team reads the blood for rejection signals, immunosuppressant levels, viral surveillance, and graft function. My endocrinologist reads it for glycemic control, thyroid status, and the metabolic effects of the immunosuppressants. My GP reads all of it, looking at the picture across organ systems—kidneys, liver, bone health, infection risk—with no single specialty filter applied.
The same number means different things to different physicians. An HbA1c of 6.8 tells my transplant team that the diabetogenic effects of tacrolimus and sirolimus are being managed. It tells my endocrinologist that the Rybelsus and Jardiance are doing their work. It tells my GP to keep tracking renal function, because well-controlled glucose protects kidneys that are already under pressure from tacrolimus nephrotoxicity. One number, three conversations.
The patient who understands this sits at the intersection of all three conversations. That is where informed decisions get made.
The Panels
What follows is an orientation to the tests ordered for my 18-month review—what each one is, what it measures, and why it matters specifically for a heart transplant recipient. These are not deep clinical dives; those will come in subsequent pieces. Consider this the map before the territory.
Heart Transplant Panel
Rejection Surveillance
Prospera (Donor-Derived Cell-Free DNA / dd-cfDNA)
Prospera measures the fraction of cell-free DNA in the blood that originates from the donated heart. When the transplanted organ is under stress—from rejection, primarily—its cells release more DNA into the bloodstream. That donor DNA is genetically distinct from the recipient’s, making it detectable. Measured as a percentage of total circulating cell-free DNA. A result below 0.15% is interpreted as low risk for acute rejection; at or above 0.15%, the transplant team will typically follow up with an endomyocardial biopsy to investigate further. Prospera now also incorporates a second metric—the Donor Quantity Score (DQS)—which accounts for fluctuations in total background cfDNA caused by factors unrelated to graft health (infection, recent surgery), reducing false positives by more than 37% compared to the fraction metric alone. For the transplant team, this is the frontline non-invasive rejection screen.
Anti-Donor Antibody (Donor-Specific Antibodies / DSA)
The immune system produces antibodies. In a transplant recipient, those antibodies can target the specific proteins—human leukocyte antigens (HLA)—present on the donor heart. Anti-donor antibodies, also called donor-specific antibodies, are a marker of antibody-mediated rejection risk. Their presence doesn’t mean rejection is occurring; it means the immune system has identified a target. Monitored at intervals throughout post-transplant care, DSA results are read alongside Prospera and biopsy findings to build an overall rejection risk picture.
Infection Monitoring
Transplant CMV (Cytomegalovirus)
CMV is a common herpesvirus that most people carry asymptomatically. Under normal circumstances it remains dormant. Under the weight of immunosuppression, it can reactivate—and in a transplant recipient, reactivation can cause serious illness: pneumonia, hepatitis, colitis. It has also been linked to accelerated CAV. Measured via PCR (polymerase chain reaction), which detects viral DNA in the blood, reported in IU/mL (international units per milliliter). The target is undetectable. Prophylaxis with valganciclovir is standard in the early post-transplant period; surveillance continues afterward because the reactivation risk does not expire.
Transplant EBV (Epstein-Barr Virus)
EBV, the virus responsible for mononucleosis, is another latent herpesvirus that can reactivate under immunosuppression. The concern specific to transplant recipients is post-transplant lymphoproliferative disorder (PTLD)—a serious condition in which B cells proliferate abnormally, driven by unchecked EBV activity. Also quantified via PCR in IU/mL, with the goal being low or undetectable. Both the transplant team and the GP track this one with particular attention.
TTV is a non-pathogenic virus—it causes no known disease—present in virtually everyone. Its clinical value in transplant medicine is that its concentration in the blood directly reflects the degree of immunosuppression: the more suppressed the immune system, the higher the TTV load; the less suppressed, the lower. Measured in copies/mL by PCR. The target range for balanced immunosuppression, as defined in a 2020 prospective trial published in the American Journal of Transplantation, is 10⁶ to 10⁸ copies/mL (one million to one hundred million)—below that range suggests under-suppression and rejection risk; above it flags over-suppression and elevated infection or malignancy risk. TTV is an emerging tool, part of a shift toward individualized rather than protocol-driven immunosuppression management. Many programs have adopted it only recently. The research base is still growing, but the concept is elegant: a naturally occurring virus as a living barometer of immune function.
Immunosuppressant Management
The trough level measures tacrolimus concentration in the blood just before the next dose—the lowest point in the dosing cycle, which reflects steady-state exposure. Measured in ng/mL (nanograms per milliliter). Target range for stable patients beyond the first year is generally 5–10 ng/mL, though individual programs differ; my team targets the lower end of that window at this stage. Too low risks rejection; too high risks nephrotoxicity, neurotoxicity, and metabolic complications. The therapeutic window is narrow, and the level fluctuates in ways that aren’t always immediately explicable—timing of the draw relative to the last dose matters significantly, as does diet. A few hours’ difference, or a high-dose magnesium supplement taken at the wrong time, can shift the result enough to change clinical interpretation entirely.
Sirolimus (Rapamune, Trough Level)
Sirolimus trough follows the same logic—the pre-dose nadir, in ng/mL. My team targets 6–8 ng/mL for each drug, with the longer-term plan of tapering mycophenolate as both stabilize. Sirolimus is an mTOR inhibitor rather than a calcineurin inhibitor, which is why it was added to address CAV—the two drugs work through different mechanisms and produce a synergistic immunosuppressive effect. Sirolimus is slow to reach steady state; early trough levels swing before the body settles in, which is why the initial weeks require frequent monitoring.
Blood & Metabolic Baseline
CBC with Differential (Complete Blood Count)
The CBC measures the major components of blood: red blood cells (RBC), white blood cells (WBC), hemoglobin, hematocrit, and platelets. The differential breaks the WBC count into its component cell types—neutrophils, lymphocytes, monocytes, eosinophils, basophils. Reported in cells per microliter (µL) or as percentages of total WBC. Standard reference ranges apply, but transplant recipients read these in the context of immunosuppression: a suppressed WBC can indicate over-immunosuppression; elevated neutrophils may signal infection. Both tacrolimus and sirolimus affect bone marrow function, and anemia is a recognized complication of post-transplant management.
Comprehensive Metabolic Panel (CMP)
The CMP covers a broad sweep: kidney function (creatinine, BUN—blood urea nitrogen), liver function (ALT, AST, alkaline phosphatase, bilirubin), electrolytes (sodium, potassium, chloride, bicarbonate), and blood glucose. Units vary by component: creatinine in mg/dL, enzymes in U/L, electrolytes in mEq/L. The transplant team uses this to monitor for tacrolimus nephrotoxicity and drug-related hepatic stress. The GP reads it as a systems-wide organ health check. The endocrinologist examines the glucose and kidney markers in the context of GLP-1 therapy and diabetes management. Few panels receive as much cross-specialty scrutiny.
Total cholesterol, LDL (low-density lipoprotein), HDL (high-density lipoprotein), and triglycerides. Standard cardiovascular risk markers, but carrying additional weight for a recipient with a CAV diagnosis. CAV is an accelerated form of vascular disease, and lipid management is among the modifiable risk factors—which is why statins are a standard component of post-transplant regimens. Reference ranges: total cholesterol below 200 mg/dL, LDL below 100 mg/dL (lower in high-risk patients), HDL above 40 mg/dL for men, triglycerides below 150 mg/dL. All three of my specialists have an interest in this one.
Measured in mg/dL; normal range 1.7–2.2 mg/dL. Low magnesium is extremely common in heart transplant recipients—tacrolimus causes renal magnesium wasting, meaning the kidneys excrete more than they should. This is not a trivial problem. Magnesium is a cofactor in dozens of enzymatic reactions and plays a critical role in cardiac rhythm. In practical terms: high-dose magnesium supplementation taken at the wrong time relative to tacrolimus interferes with absorption—divalent cations alter gastric conditions enough to affect how the drug is taken up. Once I understood that, my entire medication schedule was restructured to separate them. The serum levels stabilized. The transplant team flags hypomagnesemia closely, because low magnesium in a recipient already carrying CAV risk adds cardiovascular complication to the immunological picture.
Kidney Surveillance
This overlaps with the CMP but is ordered separately for more granular kidney assessment: creatinine, BUN, and eGFR (estimated glomerular filtration rate, measured in mL/min/1.73m²). eGFR above 60 is generally considered normal; chronic kidney disease is staged below that threshold. Tacrolimus nephrotoxicity is a long-term concern—arguably the most significant non-cardiac complication in long-term transplant recipients. The endocrinologist also reads the renal profile because Jardiance (an SGLT2 inhibitor) requires adequate eGFR to function safely and is contraindicated below certain thresholds.
Urine Protein Creatinine Ratio (UPCR)
A spot urine sample rather than a blood draw, but it travels with the panel. Protein in the urine is a marker of kidney damage or stress. The ratio of protein to creatinine normalizes for urine concentration, giving a reliable single-sample measure without a timed collection. Normal is below 0.2 mg/mg; values above 0.3 indicate significant proteinuria requiring investigation. In a recipient on both tacrolimus and sirolimus—each carrying renal implications—keeping a close eye on the kidneys is non-negotiable.
Endocrine Panel
Thyroid Function
TSH (Thyroid-Stimulating Hormone)
TSH is produced by the pituitary gland and signals the thyroid to produce thyroid hormone. Because I no longer have a thyroid—removed in October 2024 due to amiodarone-induced thyroid disease—my TSH level reflects how well my levothyroxine replacement dose is calibrated. Measured in mIU/L (milli-international units per liter); standard reference range is 0.4–4.0 mIU/L, though the precise target varies by patient and clinical context. My endocrinologist tracks this closely because the addition of Rybelsus has known interactions with thyroid hormone levels—GLP-1 agonists can affect thyroid function, and in someone managing replacement therapy rather than a functioning gland, the calibration is less forgiving than it would be in an intact system.
Free T3 (Triiodothyronine) and Free T4 (Thyroxine)
T4 is the primary form of thyroid hormone produced—or in my case, supplemented via levothyroxine. T3 is the active form the body converts T4 into. “Free” refers to the unbound fraction circulating in the blood: the portion actually available to cells, as opposed to the majority that circulates bound to proteins. Measured in pg/mL for Free T3 (normal approximately 2.3–4.2 pg/mL) and ng/dL for Free T4 (normal approximately 0.8–1.8 ng/dL). Together with TSH, they form a complete picture of thyroid status. Without a gland, this panel is how we confirm whether the replacement therapy is working. I also track symptoms independently: heart palpitations suggest hyperthyroid; persistent fatigue and cognitive sluggishness suggest hypothyroid. Both are signals I respond to without waiting for a scheduled lab appointment.
Glycemic Control
HbA1c reflects average blood glucose over the preceding two to three months, expressed as a percentage. For a non-diabetic, normal is below 5.7%; for a managed diabetic, targets typically fall below 7.0%. Mine came down from 7.1 to 6.8 following the introduction of Rybelsus. The transplant team reads this in the context of CAV—glycemic control is a modifiable cardiovascular risk factor, and uncontrolled glucose accelerates vascular disease in a recipient already carrying that burden. The endocrinologist reads it as the primary efficacy measure for the GLP-1 therapy. The GP reads it as a downstream marker for renal risk, neuropathy, and overall metabolic health. One number. Three conversations.
Bone & Mineral Metabolism
Vitamin D (25-Hydroxyvitamin D)
Measured in ng/mL; normal range generally 20–50 ng/mL, though some clinicians target the higher end for transplant recipients. Deficiency is extremely common post-transplant—immunosuppressants and reduced sun exposure (photosensitivity is a documented effect of several standard medications) both contribute. Beyond bone health, Vitamin D plays a role in immune regulation, giving the transplant team a reason to care independent of the osteoporosis concern. Low Vitamin D in a recipient already at bone-loss risk from corticosteroid exposure is a compounding problem, not an isolated one.
PTH regulates calcium and phosphate metabolism, and by extension bone homeostasis. Measured in pg/mL; normal range is 15–65 pg/mL. Elevated PTH—secondary hyperparathyroidism—is common in transplant recipients and is typically driven by low Vitamin D or impaired kidney function. In my case, the four small parathyroid glands that sit adjacent to the thyroid and were preserved during the thyroidectomy are now the entire story of calcium regulation. The endocrinologist and GP both follow this closely; PTH dysregulation layered on top of renal stress creates compounding risk to bone and cardiovascular health.
Measured in mg/dL; normal range 8.5–10.5 mg/dL. Calcium is regulated by PTH and Vitamin D, so the three markers are read as a set. Hypercalcemia can trigger cardiac arrhythmias—a concern with any patient, but particularly with a transplanted heart operating without vagal input. Hypocalcemia causes neuromuscular irritability. Post-thyroidectomy, calcium requires particular vigilance because the parathyroid glands can be disrupted during surgery even when the intent is preservation. Mine were preserved. The number still gets tracked at every encounter.
Life’s Blood
Bram Stoker’s Renfield muttered it to himself like a prayer: the blood is the life. He meant it literally, in the fevered logic of a man who had surrendered his sanity to a vampire. I mean it differently—though perhaps not so far removed.
The blood carries the record. Every vial drawn in the weeks and months after the transplant was a conversation between my new body and the team trying to understand it. Every number that came back told someone something. Most of the time, it told them I was still here and still managing.
Eighteen months out, the conversations have spaced out. The surveillance is lighter. But the blood hasn’t stopped talking.
The question is whether you’re listening.
Discover more from One More Beat
Subscribe to get the latest posts sent to your email.