Out of the Frying Pan
The listing came through on a Friday afternoon.
October 11th, 4:02 in the afternoon, Niles in the room. I had been officially listed for transplant—Status 2 at The Christ Hospital in Cincinnati, on an Impella heart pump, waiting. I posted to Facebook from the hospital bed. I HAVE BEEN OFFICIALLY LISTED. Three days of relative stability followed. The weekend curse returned Sunday evening but corrected pharmaceutically. Monday nearly killed me. Tuesday the right ventricle held.
By Thursday, October 17th, I had walked four laps around the ward, eaten a real lunch, and was beginning to feel like a man who might actually survive long enough to receive a heart.
Then endocrine walked in.
The Numbers
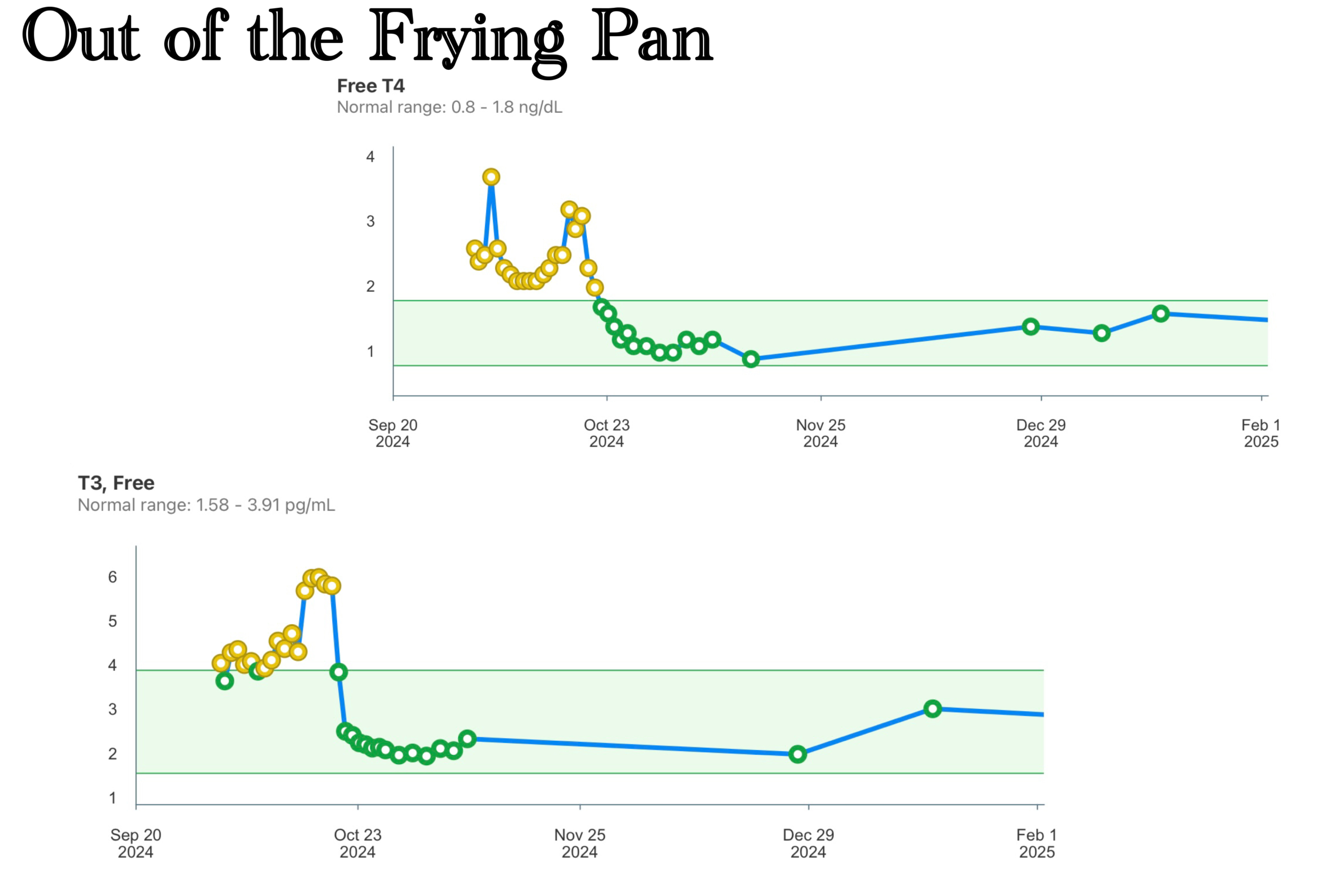
The thyroid numbers were the worst they had ever been. Not the worst in a week—the worst ever recorded in my case. The attending from endocrinology did not need to explain what that meant; I had been reading the literature for weeks. I knew what was coming, had known for some time it was coming, and I had been waiting for this shoe to drop. The runway was shortening.
The cause was amiodarone—a drug I had been on for years, given to manage the very arrhythmias that were now threatening my life. Amiodarone is thirty-seven percent iodine by weight. It is lipophilic, meaning it accumulates in fatty tissue throughout the body rather than clearing cleanly through the kidneys. Its half-life runs fifty to a hundred and forty days. Its active metabolite, desethylamiodarone, persists six to twelve months after the drug is discontinued. There is no chelation. There is no accelerated clearance. You cannot dialyze it out in any meaningful way because it lives in the tissues, not the blood.
The thyroid, for its part, is extraordinarily efficient at concentrating iodine. That is its job. Given years of amiodarone exposure, it had been saturated—and it had responded by going into toxic overdrive, producing T3 and T4 at levels that threw my heart into chaos on a schedule that had come to feel like a law of nature.
We had checked it in June. It was fine in June. Two months later it was trying to kill me.
I’m just pissed.
Dowling’s Argument
Dowling came in the next morning.
His position was direct and it was correct: putting a donor heart into a body with a thyroid in full toxic storm was out of the frying pan and into the fire. The new heart would face the same hostile endocrine environment that had been destabilizing the old one. The arrhythmias would continue. The transplant could fail. The thyroid had to go first.
They had tried prednisone—standard protocol for amiodarone-induced thyrotoxicosis. It had failed. Radioactive iodine ablation, the other standard option, was blocked by the amiodarone itself; the drug that had caused the problem was also preventing its treatment. The math was simple and there was only one answer to it.
But simple math and an easy decision are not the same thing.
The delisting was what hit hardest. Not the surgery itself—I had already concluded weeks before the surgeons recommended it that the thyroid had to go. It was being dropped from the list, even temporarily, even for a day or two, that felt like the floor had dropped out. The clock I had been watching obsessively would restart. Every day off the list was a day the runway shortened.
I was officially placed in paused status. Status 7.
The Scope
Before they could schedule the thyroidectomy, the ENT surgeon needed to examine the vocal cords. The thyroid sits directly adjacent to the recurrent laryngeal nerves—the nerves that control the vocal cords—and any surgery in that territory carries risk. Standard pre-operative protocol.
He put a scope through my nose and into my throat, had me make sounds, and watched what moved.
The left vocal cord did not move. It hadn’t been moving for weeks, it turned out. The paralysis was already there; the scope had simply confirmed what had been hiding in plain sight.
The cause remains honestly uncertain. Two theories. The first: the swan catheter inserted at Mercy West during my initial hospitalization—the recurrent laryngeal nerve runs in close proximity to the insertion path, and a nick during a procedure performed under difficult conditions on a deteriorating patient would not have been unusual. The second: the violent vomiting just before I went to the hospital—the force of it can occasionally damage the nerve. I had attributed my voice loss at the time to acid from the vomiting. I’m not certain that was wrong. I’m not certain it was right either.
Then I asked him about prognosis.
He paused before answering—not evasively, but carefully. Many times, he said, these things resolve on their own over the course of a year. Others require therapy and may improve partially or not at all. The case was not hopeless. He did not want to offer false hope either.
I asked him specifically about singing.
He gave me the same honest answer. Possibly. Possibly not. Time would tell.
The paralysis also meant the upcoming surgery carried a specific risk: if the surgeon nicked the right nerve and the second cord went, I would wake up trached. No voice. No airway of my own.
The Decision
I asked him if he was good at what he did.
He said yes. Very good.
I asked him if that was going to happen.
He said no.
I told him to get it on the schedule.
He was visibly surprised. I was told later he mentioned it to colleagues; someone on the team brought it up to me afterward. Under these conditions, most patients hedge. They ask for time. They want to discuss it further, sleep on it, call someone. The combination of circumstances alone—listed for transplant, just survived a near-death cardiac episode, about to have my throat cut with one vocal cord already gone—would seem to warrant some measure of visible deliberation.
I want to be clear about something, because it matters for anyone reading this who did not respond the way I did: the normal reaction is not weakness. Most people in that room, in that situation, would take time. Would need time. Would be right to take it. I am an outlier in this regard and I know it. The decisiveness is not a virtue I cultivated—it is simply how I am wired. I gathered the salient facts. I evaluated them. I made the decision. The hemming and hawing is not in my nature and never has been; it has simply never been more conspicuous than it was in that room.
The Only Moment of Despair
Somewhere in this window—I cannot pin the exact day—a Billy Joel song came on.
I closed the door.
I tried to sing along.
What came out was a growl. One cord working, the other silent, and what should have been a voice was something else entirely—functional enough to whisper, not functional enough to sing.
I am a singer. Have been since I was young. I have the range and I have the pipes, or had them, and music has always been a thing I did without thinking about it, the way some people walk or breathe or talk with their hands. It was not a hobby. It was part of the furniture of who I am.
What followed was the only true moment of despair I experienced throughout the entire ordeal.
I called out to the universe—whatever you do, do not take my voice. Life without song, without the ability to make music, was not life at all to me. Everything I had been through to that point, everything still to come, paled in comparison to this one thing. I meant it completely.
I gave myself the moment. Then it was over. I did not return to it.
Rabbi Nachman of Breslov taught that despair is not permitted—not as comfort, but as an instruction. You are allowed your grief. You are not allowed to live there. I had not read that teaching yet at the time, but I already knew it in my bones. The dark humor that had carried me through six weeks of medieval torture, the irreverence in the face of things that could kill me—these were not affectations. They were the mechanism. You run this thing serious and you are finished. The gallows humor is not avoidance; it is the difference between a man who endures and a man who doesn’t.
Give yourself the moment. Then get back to work.
The Buspar Negotiation
The transplant team had been watching.
They told me they were impressed—genuinely, not as flattery—at how well I was managing under conditions that typically produced far more visible deterioration. Most patients, they said, were on psychiatric support well before the six-week mark. I had declined the initial offer, made around the time of the first major AFib event. I was managing through intellect. The emotional side was spent but contained. I did not want to alter my brain chemistry when my brain was the primary instrument keeping me functional.
Dowling made the eventual argument—not as a prescription, not with any clip or impatience, but as a conversation between equals, which is how he always treated me. He was concerned for my well-being. The weeks could become months. The transplant would come. And the post-operative period would be harder than anything that had come before it—the pain, the immobility, the medications, the uncertainty, the slow grinding return to function. By then, he said, it would be too late to ramp up. There was no shame in taking the assist. Most took it far sooner.
He was right. I agreed.
I should note: somewhere in the medication management during this period, a dosage change was made without my knowledge. I gave the responsible party—not Dowling, not the transplant team, an attending from elsewhere—holy hell. Under no circumstances were they permitted to make any medication change without discussing it with me first. I was to be kept fully informed of everything happening to my body. They apologized. They did not make that mistake again.
The coda to this story: the day after the transplant, the Buspar disappeared from my medication list. No discussion. No taper. No conversation at all. Just gone.
I have chosen to find this funny.
October 19th
They took me back at 7:30 in the morning. They had scheduled four hours—extra time to be careful around the nerves.
My mother couldn’t drive in the dark, so she came up when it got light. She was in the cardiovascular waiting room while they worked. I had told them she would be there; Dr. Hellmann or someone from the team would come out when it was done.
It took about four hours. The surgeon was careful. He was as good as he said he was. The right cord was untouched. No tracheotomy.
They found nothing unexpected—no cancer, nothing unusual. Just a gland that had been saturated with iodine and had responded the only way a thyroid knows how.
I came out in a lot of pain. The incision across my throat looked, in my own estimation and by general consensus, like something from a horror movie. Halloween was two weeks away. The nurses thought this was a riot. The surgeon, when informed of the comparison, was somewhat less enthusiastic.
The Morning After
At 4:48 in the morning on October 20th, I was awake and looking at my lab results on my phone.
The T3 and T4 numbers were in free fall. Faster than I had expected—faster than anyone had anticipated. The organ was gone and the body was already responding, already beginning to recalibrate. The production line had been shut down.
I texted my mother: Woah…that thyroidectomy did its job.
The pain from the incision was rough—dilaudid, warm broth sipped carefully to quiet the throat. I was on liquids, working toward soft foods.
But something had shifted. The thyroid was gone. The accelerant was gone. The hormone storm that had been throwing my heart into AFib on a schedule so reliable it felt like a law of nature would not be happening again.
I texted my mother at 5:04 in the morning:
The heart is on its way again. I can feel it.
She said she knew it wouldn’t be long.
I was relisted the following Monday. Status 2, restored. The clock started again. The waiting resumed—but from a different position now, with a body that had been stripped of one more thing it didn’t need and was, for the first time in weeks, heading in the right direction.
Most thyroidectomy patients go on levothyroxine alone—synthetic T4, which the body converts to active T3. Given the complexity of my case, they added liothyronine as well: direct T3 supplementation, taken in the middle of the night when I wake, timed for the hours when the body’s demand is highest.
One more pill. One more 2am alarm.
I took it.
Discover more from One More Beat
Subscribe to get the latest posts sent to your email.