Buying Time: The Impella
On the morning of October 3rd, 2024, I sent a text to my buddy Eric. I told him things had taken another downturn. That afternoon they were going to implant a temporary LVAD. I told him I might not come back from this.
He responded the way Eric responds: with a bad joke about the Six Million Dollar Man, followed by something that cut straight through. One minute, one hour, one day at a time.
I went to the OR a few hours later.
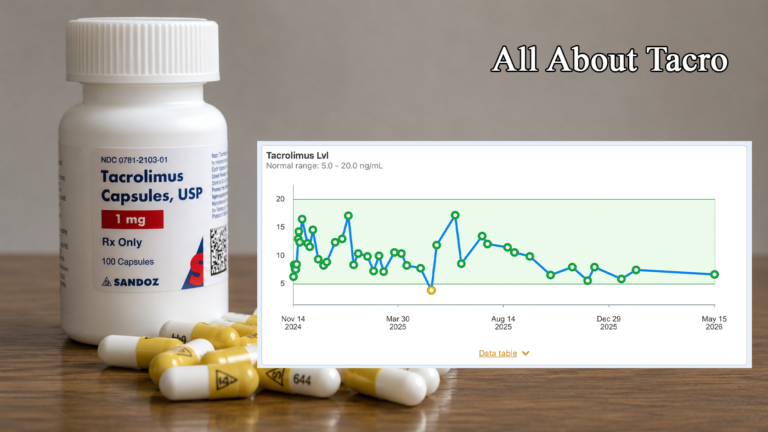
What they actually implanted that afternoon was not an LVAD. It was an Impella 5.5 with SmartAssist—a temporary mechanical heart pump, the current generation of a device that has become one of the most significant advances in mechanical circulatory support of the past two decades. The distinction between an Impella and an LVAD matters, and we will get to it. What mattered that morning was simpler: two days earlier, the options on the table were transplant, LVAD, or death. The Impella opened a door between the first two.
It kept me alive for a month. My ejection fraction at the time was approximately 5%. At that level of cardiac function, sustained survival without mechanical support or transplantation was not a realistic prospect. The Impella changed that calculation.
What It Is
The Impella is a temporary mechanical circulatory support device—a catheter-based pump that does the work a failing left ventricle can no longer do adequately on its own. It is not a replacement for the heart. It is a rest for it.
In the bridge-to-transplant context, the goal is straightforward: buy time. Keep the patient alive and hemodynamically stable while a donor heart becomes available. Every day the Impella is running is a day the transplant team has to find the right match. In my case, that was thirty-seven days.
How It Works
The Impella’s pump sits across the aortic valve, positioned with its inlet inside the left ventricle and its outlet in the ascending aorta. A rotating microaxial impeller—spinning at up to 51,000 RPM—pulls blood continuously from the left ventricle and expels it forward into the aorta, effectively bypassing much of the work the compromised heart would otherwise have to do.
This accomplishes two things simultaneously. First, it provides hemodynamic support—restoring cardiac output to levels the failing heart can no longer generate on its own, which means the kidneys, the brain, and every other organ that has been running on insufficient perfusion begin receiving adequate blood flow again. Second, it unloads the left ventricle—reducing the pressure the ventricle has to work against, which reduces myocardial oxygen demand and gives the heart muscle a chance to rest rather than continue laboring against impossible odds.
The Impella 5.5 with SmartAssist is the surgically implanted version of the device, designed for long-duration support. It delivers up to 5.5 liters of flow per minute—sufficient to sustain a patient through weeks of support while remaining mobile enough to walk. The SmartAssist technology provides real-time physiologic monitoring and hemodynamic data that assists the clinical team in managing pump function and positioning, reducing the risk of suction events that can occur when the ventricle contracts against the device’s inlet.
Insertion requires a surgical cutdown—in my case through the axillary artery in the chest and shoulder region rather than the femoral artery in the groin. The axillary approach is more surgically complex but has a meaningful advantage: it allows the patient to ambulate. Walking the halls of the cardiac ICU with an Impella in place is not comfortable, but it is possible, and physical activity during a weeks-long hospitalization matters enormously for what comes after. The stronger you are going into the surgery, the better the outcomes.
The device connects externally to the Automated Impella Controller—the machine I was tethered to for the duration. A 10.4-inch display monitors pump function in real time. It mounts to a cart for transport within the hospital. Wherever I went, it came with me, connected by approximately five feet of cord. That included the walks around the CVICU floor, the hospital halls, the outside decks, and every single procedure I had thereafter…everywhere.
A continuous purge system runs glucose solution through the catheter to prevent blood from entering the motor housing. The purge cassette requires periodic changing. This is relevant to the lived experience of the device in ways addressed below.
The support level is adjustable. The device operates on a scale, and the clinical team can dial it up or down based on hemodynamic need and patient tolerance. Dialing it down has a cost: less cardiac support. Sometimes that cost is worth paying.
The Insertion
I went to the OR on the afternoon of October 3rd and woke up with the device already in place. Thirteen staples closed the incision. The area around it would remain sensitive for weeks—not dramatically painful but persistently present, a reminder with every movement that something significant had been done there.
The staples came out on October 27th. That was twenty-four days after insertion. The nurse almost forgot. I had no intention of reminding her. (Sam gave me a hard time about that and called me a big baby when I reacted to the staples coming out; it really didn’t hurt, I was just being dramatic.)
Living With It
What nobody tells you before the Impella is placed is what it is like to actually live with one for weeks.
The machine is constant. The Automated Impella Controller sits on its cart, connected to you by cord, present in every corner of the room, accompanying every walk down the hall, occupying the space next to the bed at 3am with the same indifferent persistence it occupies it at noon. You push it ahead of you when you walk. You navigate it around furniture. You develop a permanent low-level awareness of the cord—where it is, what it might catch on, what happens if you turn wrong. Nothing catastrophic happens if you turn wrong. The device is more securely anchored than your nervous system is willing to accept at 3am. But the anxiety does not entirely care about that.
The machine makes noise. A continuous mechanical whir that becomes background within a day or two—until it changes pitch in the middle of the night, which it does with some regularity, and then it is not background at all. The variations are not necessarily alarming in the clinical sense. They are alarming in the 3am sense, which is a different and more persistent category.
Then there are the purge cassette changes. These happen periodically, and the sound the device makes during the process—a rhythmic kerchunk-kerchunk-kerchunk that arrives without warning, usually somewhere around 2am—is not a sound that invites calm reflection on one’s circumstances. When the cassette does not quite seat correctly on the first attempt, the process takes longer than it otherwise would. The nurses were considerably more accustomed to this than I was. That gap in composure was noticeable.
The dressing at the insertion site is changed regularly. The skin around an Impella insertion site is sensitive, and infection risk is real—an infected insertion site is a serious complication that can significantly complicate patient management. The nursing staff takes dressing changes accordingly. One nurse in particular applied dressings with the thoroughness of a field medic preparing for a six-month deployment in hostile terrain. Those things were engineered to last. I teased her about it regularly. I was also genuinely grateful.
The Clinical Side Effects
Thrombocytopenia—low platelet count—is a documented adverse event associated with Impella use. The rotating impeller mechanically shears platelets as blood passes through the device. This is not an edge case; it is a known and expected consequence of how the device works, and the clinical team monitors platelet counts accordingly.
In my case, the effect was tangible. Persistent nosebleeds. Platelets taking what the records from that period accurately describe as a significant hit. On October 21st, the device was dialed back one support level specifically to help the platelet count recover. The reduction in support level was perceptible almost immediately—not dramatically, but distinctly. That is the tradeoff: less platelet shearing in exchange for less cardiac support. The patient experiences it as a choice between two kinds of not quite right.
Hemolysis—the mechanical breakdown of red blood cells—is a related adverse event associated with mechanical pump use, operating through similar mechanisms. It is worth knowing about and worth asking the care team to monitor.
The Cognitive Shift
Severely compromised cardiac output means the brain has been running on insufficient blood flow. The patient does not fully know this is happening. The fog becomes the baseline. It is all they have known for however long the heart has been failing—weeks, months, years in some cases. The cognitive impairment does not announce itself. It simply becomes the new normal, invisible from inside it.
When the Impella restores adequate cardiac output, the fog lifts. Sometimes quickly. The brain, receiving blood flow it has been starved of, begins operating differently.
My friend Niles saw it from the outside. He described the difference as striking—observably, significantly different from one side of the device placement to the other. I cannot fully report my own before-and-after because I was inside both states. That is the nature of it: the patient is the least reliable observer of their own cognitive recovery in this situation, because the compromised state affected the very faculties needed to assess it. The people around them are the better historians.
This is one of the reasons the informed caregiver matters. They are watching something the patient cannot see. For more on what the hospitalization looks like from the other side of the bed, the Caregivers Cornerseries (live 6/21/2026) on this site addresses the caregiver’s experience directly.
Impella vs. LVAD—The Decision
When both options are on the table, the considerations differ significantly.
An LVAD—Left Ventricular Assist Device—is a surgically implanted pump designed for long-term or permanent support. It involves a more extensive surgical procedure, an external controller and power source connected via a driveline that exits the body, and a significant ongoing lifestyle adjustment. Patients on LVADs go home. They live with the device for months or years. The commitment is substantial.
The Impella is a shorter-commitment bridge. FDA-approved for up to fourteen days, it is used longer in bridge-to-transplant scenarios under clinical judgment and institutional protocols—in my case, thirty-seven days. It does not go home with the patient. It is a hospital-based intervention designed to buy time until the next step is available.
When the goal is getting to transplant rather than long-term mechanical support, that distinction matters considerably. This is not a clinical recommendation—it is a framework for understanding the conversation with the care team, who will make the determination based on hemodynamic need, anatomy, institutional experience, and the specific clinical picture in front of them.
The Bottom Line
An ejection fraction of approximately 5%, in the context of end-stage heart failure, was not a situation that could continue without intervention. The Impella 5.5 provided the cardiac output my heart could not, for thirty-seven days, while a donor heart became available.
It is not comfortable. The noise, the tether, the dressing changes, the nosebleeds, the kerchunk-kerchunk-kerchunk at 2am—none of it is comfortable. It is also, without meaningful exaggeration, the reason I am writing this.
Eric lost the lunch bet and, for the record, I collected in the spring of my second year post-op. He treated to a German bier-garten. It was a great lunch.
For comprehensive information on the Impella device and its clinical applications, Abiomed’s Heart Recovery site provides the most complete overview available. Noted here as the manufacturer’s resource; clinical claims in this piece are drawn from peer-reviewed literature and direct patient experience.
Discover more from One More Beat
Subscribe to get the latest posts sent to your email.