All About Tacrolimus
A note before we begin: The goal of this piece is to make you a better-informed participant in your own care — not to replace your transplant team. They know your numbers, your history, your other conditions, and your specific risk profile in ways no article can. They are the experts. What follows is context for the medication they are managing: where it came from, how it works, what the monitoring numbers mean, what moves those numbers, and what the real side-effect landscape looks like. Use it to have better conversations with the people who are actually prescribing for you.
You came home from the hospital with a pill bottle. The label says tacrolimus. The instructions are precise and presented as non-negotiable: twice daily, same times every day, on an empty stomach or consistently with the same type of meal, do not miss doses, do not take with grapefruit. The label does not explain why any of that matters, what the drug is actually doing inside you, what the team is watching when they order trough levels, or what the long-term stakes are if those levels drift in either direction.
This is that conversation.
Where It Came From
In 1984, researchers at Fujisawa Pharmaceutical (now Astellas) sampling soil from the Tsukuba region of Japan isolated a bacterium, Streptomyces tsukubaensis. From its fermentation broth they extracted a macrolide compound they called FK506. It had antifungal properties. Its more interesting effect turned out to be potent suppression of immune activity.
The compound was renamed tacrolimus and marketed under the trade name Prograf. An extended-release formulation, Envarsus XR, was developed later from the same active molecule. FDA approval came first for liver transplantation in 1994; heart transplantation followed as accumulating clinical evidence demonstrated consistent advantages over the previous standard agent, cyclosporine — approved in 1983 and the first drug to make transplant medicine genuinely viable at scale.
Tacrolimus is generally considered roughly 10–100 times more potent than cyclosporine on a weight basis, and in head-to-head transplant studies it produced lower rates of acute rejection. Over roughly a decade it largely displaced cyclosporine as the dominant immunosuppressant in heart recipients. This piece focuses on immediate-release Prograf — the twice-daily capsule still most commonly initiated in heart transplant — because that is what most newly transplanted patients will encounter first. The extended-release versions have different pharmacokinetics and different food effects; they are not directly interchangeable with Prograf and are not covered here.
(One additional wrinkle: while Envarsus and Prograf are not interchangeable, generic immediate-release tacrolimus formulations are widely used and generally perform well. Because tacrolimus has a narrow therapeutic window, many transplant centers prefer patients remain on the same manufacturer whenever possible. If your pharmacy switches suppliers, make a note of it. Most of the time nothing happens. Occasionally it becomes a useful clue when a trough level moves in a direction nobody expected.)
What It Does — And How
The transplanted heart is foreign tissue. Your immune system is exceptionally good at recognizing foreign tissue and preparing to attack it. Without intervention, it would. Tacrolimus is the primary agent standing between your immune system and that new heart.
The next few paragraphs get into the mechanism. If you are here for practical management information, skip ahead to “The Trough.” If you want to understand why the rules around timing, food, and drug interactions exist — and why the side effects are what they are — keep reading. This is worth knowing.
Your immune system’s main attack cells are T-lymphocytes, or T-cells. When they encounter tissue they identify as foreign — including your donor heart — a chemical signaling chain fires that tells those cells to multiply and mobilize. A key enzyme in that chain is calcineurin. When calcineurin is activated, it switches on a protein called NFAT, which in turn tells the cell to produce interleukin-2 (IL-2) — essentially the “go” signal that drives T-cell proliferation and launches the immune response.
Tacrolimus works by binding to a protein inside the T-cell called FKBP-12. The resulting combination blocks calcineurin. No calcineurin means no NFAT signal, no IL-2, and no organized T-cell assault on the graft. The immune system doesn’t forget the heart is there. It simply loses the ability to mount a coordinated attack against it.
Here is the part that explains nearly everything about this drug’s side-effect profile: calcineurin is not only found in T-cells. It is present in kidney cells, in the insulin-producing beta cells of the pancreas, and in neurons. Blocking it system-wide is the reason tacrolimus works — and the reason it produces the side effects it does. It is not a targeted strike. It is a very effective intervention with broad consequences that have to be managed.
A useful way to think about it: tacrolimus doesn’t disarm the immune system’s soldiers. It cuts the communication line between threat-detection and the response. The army is still present. The orders to mobilize against the graft don’t get through.
The Trough — How Centers Monitor It
Because tacrolimus has a narrow range where it’s effective without being harmful, its level in the blood has to be measured regularly. The standard measurement is the trough — the concentration in your blood at its lowest point, just before the next scheduled dose.
The blood draw for a trough is timed before you take your morning medication. That timing is not incidental — taking the pill before the draw would produce an artificially elevated result and make the number meaningless. The trough is the minimum level present across the dosing interval, and it’s the value that correlates most reliably with both preventing rejection and avoiding toxicity. This is why transplant clinics are full of people carrying pill organizers they are not allowed to open yet. Virtually every transplant center uses trough monitoring for this reason. Peak levels, which occur an hour or two after dosing, vary too much based on gut function and what you ate to be consistently useful.
Target ranges vary by center and by how far out from transplant you are. General benchmarks from the clinical literature:
• Early post-transplant (roughly the first one to six months): most centers aim for 10–15 ng/mL. Rejection risk is highest while the immune system is at full strength and the graft is most vulnerable.
• Later (six months and beyond): targets typically step down to 8–12 ng/mL, then often to 5–10 ng/mL as stability is established and the rejection risk decreases over time.
These are population benchmarks. Your team may hold you higher or lower for reasons specific to your situation — a prior rejection episode, a kidney function concern, an infection that changes the calculus. The number on your lab report is not your prescription.
Levels are reported in nanograms per milliliter (ng/mL). The general reference range on most lab reports spans a broad 5.0–20.0 ng/mL. Your therapeutic target is a narrower band inside that.
A word on missed doses. Tacrolimus isn’t stored in large reserves in your body. The level drops relatively quickly when a dose is missed, which is why a single missed dose can move the number meaningfully. A single missed dose, if caught promptly and handled the way your team instructs, is usually not catastrophic.
A pattern of missed doses is a different situation entirely.
The drug doesn’t let you make it up later.
What happens at the extremes:
• Too low: immunosuppression becomes inadequate. The immune system begins to act on the graft. Acute rejection can develop without announcing itself — fatigue, shortness of breath, and fluid retention are possible signs, but structural damage to the heart tissue can be underway before those appear. Endomyocardial biopsies and newer blood tests like donor-derived cell-free DNA (dd-cfDNA, commonly measured by the Prospera assay) exist precisely to catch subclinical rejection before it becomes symptomatic. The biopsy schedule is not administrative. It is how rejection gets caught early.
• Too high: the drug becomes the problem. According to the Prograf prescribing information, supratherapeutic levels intensify nephrotoxicity, neurotoxicity, and the full side-effect profile described below. The kidney damage in particular accumulates. Chronic kidney disease is one of the most significant long-term complications after heart transplantation, and tacrolimus is the primary pharmacologic driver. Teams therefore aim for the lowest level that provides adequate protection — not the highest level that stays in range.
The Adjustment Phase — What It Actually Looks Like
There is no reliable formula that predicts exactly what oral dose will produce a target trough in a given patient. Body weight, gut function, liver metabolism, concurrent medications, diet, and individual genetic variation in how the drug is broken down all influence the result — and they interact with each other in ways that are not fully predictable from the outside. Part of that variation is genetic: people differ in how actively their bodies express the enzyme (CYP3A4/ CYP3A5) that metabolizes tacrolimus, which is part of why the same dose produces different levels in different patients.
Teams start with a weight-based protocol dose and use the trough as feedback to dial in.
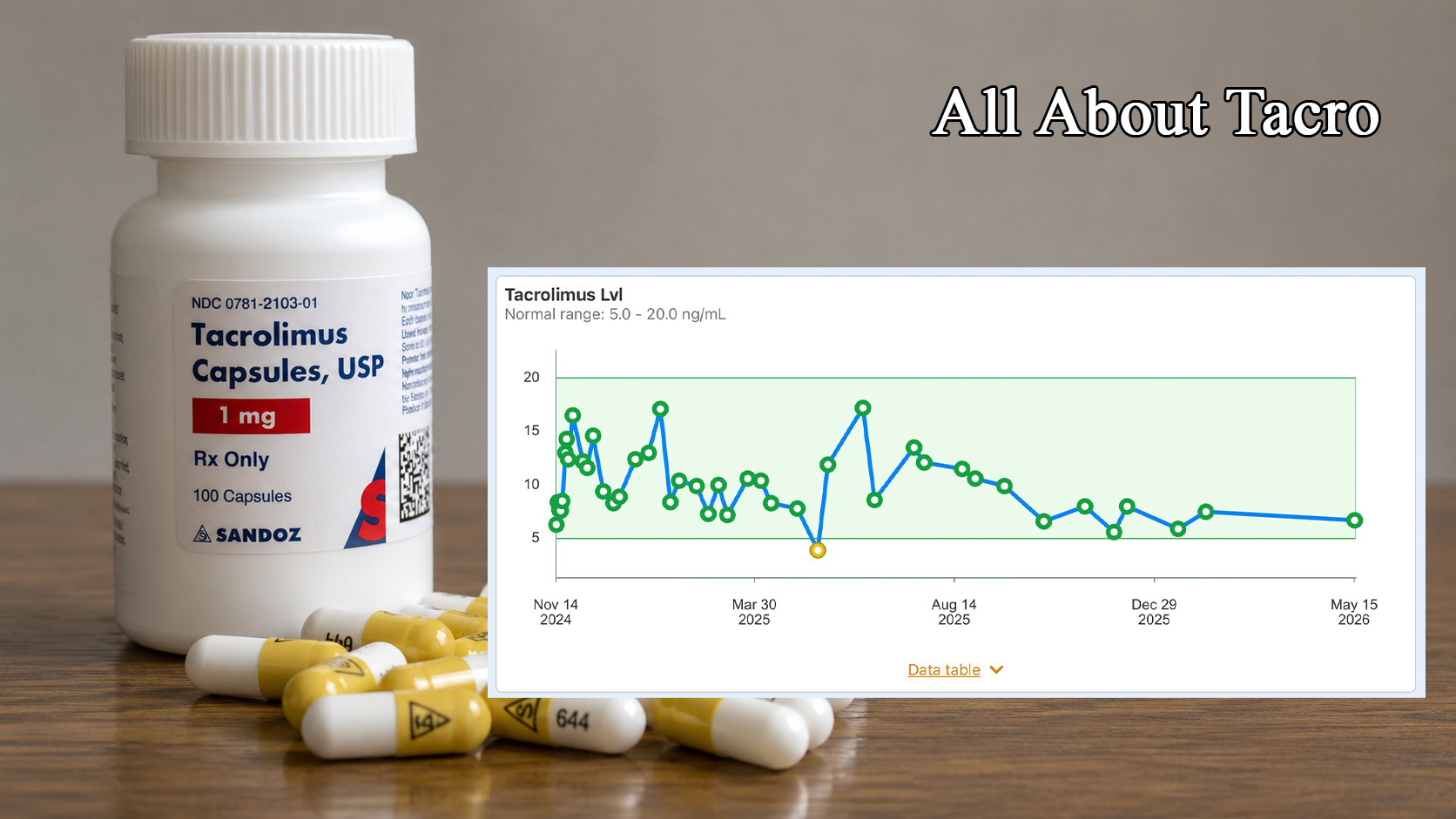
What that process looks like in practice: five days after transplant, one recipient’s level came back at 6.3 ng/mL — low for that high-risk early window. Over the following ten days, as the dose was increased, the level climbed through 8.4, 13.0, 14.3, reaching 16.5 ng/mL. Then the seesaw characteristic of early titration: 12.4, back to 11.6, 14.6, dropping to 9.4. In early January a level of 17.1 — the team had pushed the dose to compensate for a period when levels ran lower than intended. They backed off; the level walked down through spring.
Six months post-transplant the level dropped to 3.9 ng/mL, flagged as low. The first assumption from the team was missed doses — a reasonable clinical reflex, since non-compliance is the most common explanation for a sudden, unexplained drop. It was a reasonable assumption. It was also wrong.
The doses had been taken consistently; what had changed was diet composition and the timing of magnesium supplementation relative to the tacrolimus dose. Both affect how much tacrolimus actually gets absorbed. Once those variables were identified and corrected, the level responded. The team briefly overcorrected (17.2 ng/mL the following month), and from August onward the level has lived in the 6–10 ng/mL range.
You are the only person in this arrangement who is present for every dose, every meal, and every supplement. The team works from lab values and the history you report. When the numbers don’t match expectations, your detailed knowledge of your own behavior is clinically relevant data. Advocating for investigation of non-compliance explanations when you know compliance is not the issue is part of informed participation — not being difficult.
The monitoring cadence (general pattern; your center may vary):
• First weeks post-transplant: daily or near-daily draws while levels are moving quickly and stakes are highest.
• First few months: at every clinic visit, often weekly or every two weeks.
• Later: monthly, then quarterly as stability is established.
• Any dose adjustment resets the cadence temporarily, back to more frequent monitoring until the new level stabilizes.
If you are newly discharged and getting what feels like constant blood draws, that is exactly why.
What Moves the Level
Tacrolimus levels are not fixed. They respond to what you eat, when you eat it, what else you take, how your gut is functioning, and what other medications are in the stack. Understanding the main variables is part of managing this medication intelligently.
Fat content and timing. A 2001 study in the Journal of Clinical Pharmacology established that taking tacrolimus with a high-fat meal reduces the amount absorbed by roughly 35–40%, with a significant delay in the time it takes to reach peak concentration. The drug doesn’t disappear — it partitions differently in the gut and less reaches the bloodstream. What matters most is consistency: taking it fasted every day, or always with the same modest-fat meal, produces more predictable levels than alternating between fasted days and high-fat-meal days. The variability is the problem, not any single approach.
The CYP3A4 pathway. Tacrolimus is broken down in the gut wall and liver by an enzyme called CYP3A4. Anything that inhibits this enzyme slows the breakdown of tacrolimus and allows it to accumulate — levels rise. Anything that induces or speeds up this enzyme accelerates the breakdown — levels fall. This is the mechanism behind most of the food and drug interactions, covered in depth in What to Avoid and Why. The short version:
• Things that raise levels (CYP3A4 inhibitors): grapefruit and closely related citrus — the active compounds can inhibit the enzyme for up to 72 hours from a single glass, according to research published in Clinical Pharmacology & Therapeutics; pomegranate; certain azole antifungals commonly prescribed to transplant patients (fluconazole, voriconazole — teams know this and adjust doses when these are started); some calcium-channel blockers (diltiazem, verapamil).
• Things that lower levels (CYP3A4 inducers): St. John’s Wort, strong enough to be considered an absolute contraindication in transplant recipients — it can substantially lower tacrolimus levels and has been associated with rejection risk; rifampin, an antibiotic used for tuberculosis; certain anticonvulsants including phenytoin and carbamazepine.
Any time a new medication is added — especially an antibiotic or antifungal — it is worth confirming with your team whether it has meaningful CYP3A4 activity. This is not a conversation to delay.
Magnesium supplementation timing. Magnesium-containing supplements can interfere with tacrolimus absorption when taken close together, which is why many centers recommend separating them by several hours. The practical consequence is that taking a large magnesium dose with your tacrolimus consistently can blunt absorption in a way that produces low trough levels — the kind that look like missed doses but aren’t. Spacing them out is the straightforward fix. The full discussion of magnesium supplementation — forms, doses, timing — is in the Magnesium piece.
GI illness and diarrhea. This one surprises people. Acute diarrhea or gastroenteritis typically increasestacrolimus absorption, not decreases it. When the gut is inflamed or hypermotile, the normal metabolic processing in the gut wall is disrupted, and more tacrolimus passes into the bloodstream unmetabolized. The result can be a spike in levels at exactly the moment you might expect them to drop. Any significant GI illness is a reason to alert your team and watch the levels more closely until things normalize.
The Side Effects — The Real List
The prescribing information for tacrolimus lists a long catalog of possible adverse effects. Not everyone experiences all of them; most people experience some of them. What the label doesn’t always convey is the why — and understanding the mechanism makes the side effects easier to anticipate, recognize, and discuss with your team. According to the Prograf prescribing information, these are the ones that matter most for heart recipients.
Tremor. The most common neurological side effect, present in 48–56% of recipients. It shows up as a fine shake in the hands — most noticeable when holding something still, pouring a drink, or doing anything requiring a steady hand. It is a direct consequence of calcineurin inhibition in neurons — the same pathway blocked in T-cells is partially blocked in the nervous system. At therapeutic levels it is usually manageable and tends to improve as doses are lowered over time. At elevated levels it becomes more pronounced. If the tremor is new or worsening, that is worth reporting to the team.
Paresthesia. Reported in 17–40% of recipients according to the prescribing label — numbness, tingling, or burning sensations, typically in the hands and feet. Like tremors, it is a direct consequence of calcineurin inhibition in the nervous system, affecting peripheral nerve signaling rather than motor function. It tends to be most pronounced when levels are highest and often improves as doses are reduced over time. It is worth mentioning to your team if it appears, both because it is manageable and because worsening paresthesia can be an early signal that levels are running high.
Insomnia. Reported in 32–64% of recipients — a wide range that reflects how much individual response varies. The mechanism is not fully established but involves both the neurological effects of calcineurin inhibition and the broader sleep disruption that comes with the post-transplant medication regimen generally. It can be genuinely resistant to standard sleep interventions.
Hair changes. Not listed with a frequency in the core FDA label, but a 2005 study in Transplantation found clinically significant hair loss in approximately 29% of tacrolimus-treated recipients, versus none in a cyclosporine-treated comparison group. (Cyclosporine frequently causes hirsutism, excessive body/facial hair growth.) The mechanism involves tacrolimus’s effect on hair follicle cycling. In most cases it is a temporary phase; hair returns, often with changes in texture or thickness. A skull shaver is a reasonable contingency plan. It may not be needed.
Magnesium depletion. Present in 16–48% of recipients. Tacrolimus impairs the kidney’s ability to hold onto magnesium, which is then lost in urine rather than retained. The result is chronic depletion that requires active supplementation and regular monitoring. Low magnesium produces muscle cramping (particularly in the legs and hands, and particularly at night), disrupted sleep, anxiety-like symptoms, cognitive fog, and its own fine tremor that can be difficult to distinguish from the tacrolimus-induced tremor. The full treatment of this — why it happens, how to supplement correctly, and why the form of magnesium matters — is in the Magnesium piece.
Kidneys — nephrotoxicity. This is the long-term consequence that matters most. Tacrolimus causes the blood vessels feeding the kidneys to constrict, reducing blood flow and filtration. Over months and years, this chronic reduction contributes to scarring and loss of kidney function. ISHLT registry data identify chronic renal dysfunction as one of the leading long-term complications after heart transplantation, and tacrolimus is the primary pharmacologic driver. Teams monitor kidney function at every lab draw — creatinine, estimated glomerular filtration rate (eGFR), and the renal panel — and try to keep tacrolimus at the lowest effective level whenever rejection risk permits.
The kidney and the heart are in constant negotiation here.
Diabetes — the diabetogenic effect. Tacrolimus blocks calcineurin in the pancreatic beta cells responsible for producing insulin. This is a direct impairment of insulin secretion — distinct from the insulin resistance caused by sirolimus or the blood-sugar elevation caused by corticosteroids. Hyperglycemia is listed among the most common adverse reactions in the Prograf prescribing information, affecting a substantial portion of recipients—with rates varying depending on the transplant population and what other immunosuppressants are on board. Post-transplant diabetes mellitus is a recognized complication affecting a substantial portion of the transplant population, and the diabetogenic burden comes from the pharmacology, not from dietary choices alone. Managing it requires glucose monitoring, honest conversations with the team about the medication stack’s contribution, and — when medication is needed — treatment calibrated to a situation that will shift as the immunosuppressant regimen evolves over time. For recipients also on sirolimus, the two drugs create a double burden: impaired insulin production (tacrolimus) stacked on top of impaired insulin response (sirolimus). It is not a simple problem, and it is not your fault.
That list is long. Read all at once, it can feel like a verdict. It isn’t. Most recipients experience some of these effects, not all of them — and of those that do appear, many are dose-dependent, meaning they tend to be most pronounced early, when levels are highest, and improve as the regimen stabilizes over time. Tremors that makes holding a coffee cup difficult in month two may be unremarkable by month six. Hair that thins between months three and nine typically returns. The paresthesia, the insomnia, the magnesium cramping at three in the morning — these are real, and they are worth reporting to your team rather than simply enduring. Your team has tools. Some of these effects can be managed directly; others ease on their own as the dose walks down. None of them should be suffered in silence on the assumption that this is just how it is now.
And then there is the harder thing to say, which is also the truest: this drug is genuinely difficult to live with. It is also, in the most literal sense, the reason you are living. For most recipients, that accounting is not a close call. The side effects are the price. The alternative is not on the table.
Why All of This Matters — The Narrow Road
The therapeutic window for tacrolimus is genuinely narrow. Below it, the graft is at risk — rejection damage, once it occurs, is often irreversible. Above it, the patient is at risk from the drug itself, particularly through cumulative kidney injury that also does not fully reverse. Unlike medications where modest dosing variation is a minor deviation with minor consequences, here chronic off-target exposure in either direction accumulates damage over time in ways that show up years later.
The food rules, the timing protocols, the drug-interaction cautions, the frequent blood draws, the dose adjustments — none of that is administrative friction. It is the practical work of staying on a very narrow road for the rest of your life. Understanding why the road is narrow is the first step to staying on it.
The Informed Patient
Understanding your medications does not make you a pharmacologist. It makes you a more useful participant in a process where you are the only person present at every dose, every meal, every supplement, and every bout of GI illness. Your transplant team consists of experts who are very good at interpreting data. The more clearly you understand what they are managing and why, the more useful the information you bring to that conversation.
The rest is their job. Do your part. Call when something changes.
Nothing in this piece constitutes medical advice. The mechanisms, frequencies, and clinical ranges cited are drawn from FDA prescribing information, peer-reviewed transplant literature, and ISHLT registry data. Your specific target range, dose, monitoring schedule, and management plan are determined by your transplant team based on your individual clinical situation. They are the ones to call.
More on these topics:
• What to Avoid and Why — the full food, supplement, and drug interaction guide
• Magnesium — depletion, supplementation forms and strategy, timing relative to tacrolimus
• The Fine Print — the broader side-effect landscape of the full immunosuppressant regimen
• The Blood Is the Life — the full post-transplant lab panel and what each value is tracking
Discover more from One More Beat
Subscribe to get the latest posts sent to your email.