Living with Immunosuppression: What the Science Actually Says
This is the companion piece to “The Year of Living Carefully” which covers what it actually felt like to live inside the constraints of an immunosuppressed state. This piece covers the clinical and biological dimensions of post-transplant immune management.
The discharge paperwork covers a lot of ground. Medication schedules. Dietary restrictions. Follow-up appointments. Warning signs. It is thorough in the way that a legal document is thorough—complete, technically accurate, and practically insufficient for understanding what the next year of your life is actually going to look like.
What the paperwork does not do is explain the biology. It tells you what to do but not why the restrictions exist, how long they apply, or how the calculus changes as recovery progresses. That gap—between the instruction sheet and the understanding that makes those instructions make sense—is what this piece is for.
Immunosuppression is not a temporary inconvenience layered on top of an otherwise normal life. It is the central organizing fact of post-transplant existence, and understanding it—what it actually does, why it is structured the way it is, and how it evolves over time—is the foundation on which every practical decision gets made.
What Immunosuppression Actually Is
The most important misconception to clear away first: immunosuppression is not the absence of an immune system. The immune system is still present. It is still working. What has changed is that it has been deliberately recalibrated—dialed back from its normal operating level to prevent it from doing what it was designed to do: recognize and destroy foreign tissue.
The transplanted heart is foreign tissue. Without suppression, the immune system would identify the donor organ as non-self and mount a rejection response. That response would be rapid, decisive, and fatal to the graft. Immunosuppression exists to prevent that outcome. The tradeoff is that the same suppression that protects the graft also blunts the immune system’s response to pathogens, aberrant cells, and environmental threats.
The distinction between immunosuppressed and immunodeficient matters enormously.
Immunodeficiency means the system doesn’t function. Immunosuppression means the system functions—but the response is slower, less aggressive, and more tightly constrained. Pathogens that a healthy immune system dispatches quickly get more time to establish themselves. Viruses that would be controlled immediately can replicate longer before the response catches up. The immune system still fights. It just fights at a disadvantage.
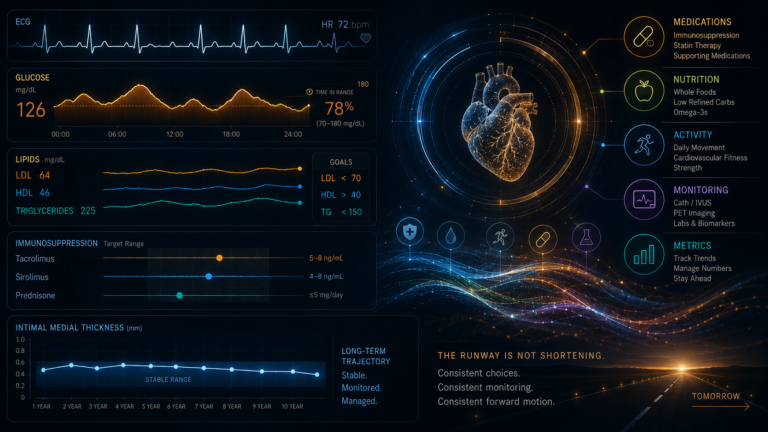
The two primary agents managing this in most heart transplant recipients work through a multi-lock mechanism. Tacrolimus—a calcineurin inhibitor—stops T-cells from activating and sounding the alarm that foreign tissue is present. Sirolimus or mycophenolate mofetil stops immune cells from proliferating even if they do activate. Two different biochemical angles, both necessary, approaching the rejection problem from different directions. Different combinations shift different risk profiles—rejection risk, kidney injury, metabolic effects, malignancy risk—which is why transplant regimens evolve over time rather than remaining static. Once the implications of being the active operational manager of a deliberately compromised immune system settle in, the biology behind every restriction begins to make its own kind of sense.
The Two Phases: Maximum Caution and Managed Vigilance
Post-transplant immunosuppression is not a single, unchanging state. It operates in two meaningfully distinct phases, and understanding the difference between them is what allows recipients to stop treating the first year’s restrictions as permanent features of their lives.
Phase One: Months One Through Nine
The first months after transplant involve the heaviest suppression of the entire post-transplant course. The graft is new. The immune system has not yet reached any accommodation with the foreign organ. The rejection risk is at its highest, and the team keeps suppression heavy to match. Tacrolimus trough targets during this period typically run 10—15 ng/mL. In my own bloodwork, the immediate post-transplant readings ran 12—16 ng/mL through the first weeks, with the team managing them downward as the picture stabilized.
This is the period of maximum caution. Masking everywhere indoors. Avoiding crowds. No high-risk environments. Strict hand hygiene. The full prophylactic medication stack running alongside the immunosuppressants. These restrictions are not overcaution—they are the correct protocol calibrated to the actual risk level of that phase.
Phase Two: Year One and Beyond
As the graft stabilizes and the rejection risk profile changes, suppression is intentionally and gradually reduced. This reduction reflects something real happening biologically: the vascular endothelium of the donor heart and the recipient’s immune system reach what might be described as a coached truce—graft accommodation, in clinical terms. The immune system does not stop recognizing the heart as foreign. It reaches a managed tolerance of it, reinforced continuously by the immunosuppressants but requiring progressively less pharmacological force to maintain.
Tacrolimus trough targets step down toward 5—8 ng/mL by year one and typically further thereafter. My own readings, now at eighteen months, run consistently in the 6—7 ng/mL range—less than half the immediate post-transplant levels. That reduction is intentional, data-driven, and reflects the team’s assessment that the graft is stable enough to tolerate less suppression. Trough targets are individualized—influenced by rejection history, kidney function, and concurrent medications—so the specific numbers vary by patient and by protocol.
The envelope of what is safe expands in Phase Two. Not because the risk disappears—it doesn’t—but because the risk calculus genuinely changes. The restrictions appropriate to month three are not appropriate to month eighteen, and treating them as equivalent is both unnecessary and costly to quality of life.
Worth naming explicitly: one of the stranger features of transplant recovery is that the psychology of vulnerability often persists well beyond the highest-risk phase. Recipients who have been in maximum-caution mode for the better part of a year don’t simply recalibrate when the trough targets come down. The behavioral patterns formed under maximum suppression can outlast the medical rationale for them. Awareness of this lag is part of navigating the second phase well.
The Prophylactic Medications: Scaffolding
Alongside the primary immunosuppressants, the first year of transplant typically involves a stack of prophylactic medications protecting against specific opportunistic infections—pathogens that a healthy immune system handles without incident and that can cause serious or fatal disease in the immunosuppressed. These medications are not permanent. They are scaffolding: present while the immune system is most vulnerable, tapered as that vulnerability decreases.
Valganciclovir (Valcyte)—CMV
Cytomegalovirus is among the most consequential infectious risks in the first post-transplant year. In immune-competent adults, CMV is a common virus—most people carry it without symptoms. In an immunosuppressed recipient, CMV can cause pneumonitis, hepatitis, colitis, retinitis, and direct injury to the graft itself. Uncontrolled, it is a serious and potentially life-threatening complication.
The highest-risk scenario is the CMV-negative recipient receiving a CMV-positive donor heart—confirmed by pre-transplant serology. The recipient arrives with no pre-existing immunity to a virus living latently in the donated organ. Valganciclovir suppresses viral replication during the period when the immune system is least equipped to do so itself. For most recipients in this pairing, prophylaxis continues for approximately twelve months.
My own CMV bloodwork illustrates what successful surveillance looks like. Clean results from transplant through most of the post-transplant period, then a brief detectable signal in January and February 2026—flagged abnormal at subclinical levels of <35 IU/mL and <2 Log10—followed by a return to not detected by May 2026. What this may represent is controlled low-level viral exposure occurring without progression to active disease—potentially part of the gradual development of CMV-specific immune control seen in some D+/R- recipients over time. The literature supports this trajectory, though it does not always proceed this way, which is precisely why PCR monitoring continues after prophylaxis ends.
Bactrim (Trimethoprim-Sulfamethoxazole)—PCP
Pneumocystis jirovecii pneumonia is caused by a fungal pathogen that immune-competent people encounter and suppress without incident. In the immunosuppressed, it can cause a pneumonia that alters gas exchange catastrophically—which is why prophylaxis during the period of heaviest suppression is non-negotiable. Bactrim is the standard agent. For most recipients it continues for approximately six months, tapering as suppression is reduced and the risk profile changes.
Antifungal Prophylaxis—Invasive Fungal Infection
The immunosuppressed lung is vulnerable to invasive fungal infections—Aspergillus primarily, but also other molds and yeasts—that a healthy immune system encounters and clears routinely without ever becoming symptomatic. These spores are microscopic, ubiquitous in ordinary ambient air, and constantly inhaled; under normal immune function they are cleared before establishing. Under suppression, they can colonize and cause serious systemic disease. Antifungal prophylaxis, typically an azole agent such as Cresemba (isavuconazole) or voriconazole, provides coverage during the highest-risk period. Duration varies by center and patient risk profile; for most recipients it runs through approximately six months post-transplant.
Why They All Eventually Stop
The discontinuation of prophylactic medications is a clinical milestone, not a routine administrative event. It signals that the team’s assessment of net immune function has reached a threshold where the system can manage these threats without pharmaceutical assistance. The scaffolding comes down because the structure can stand on its own. At eighteen months, I am off all prophylactics—valganciclovir discontinued at approximately twelve months, Bactrim and antifungals at approximately six months. That tapering tracked the reduction in suppression and the stabilization of the graft.
A Note on Vaccination
Vaccination warrants a brief but explicit mention, because its role changes meaningfully after transplant and the omission of it from most patient discussions creates real gaps in understanding.
Inactivated vaccines—the flu shot, the COVID vaccines, pneumococcal, hepatitis B, and others using killed or subunit formulations—remain important and are generally recommended for transplant recipients, with the caveat that immune response may be blunted under suppression. The vaccines can still provide partial protection and are not contraindicated; the team may time certain vaccines relative to suppression levels to optimize response.
Live attenuated vaccines—MMR, varicella, live-attenuated influenza, yellow fever, and others—are generally contraindicated after transplant. The weakened live virus in these formulations poses a real risk of causing disease in an immunosuppressed recipient rather than producing immunity.
Household vaccination is indirectly protective. A family member or close contact who is vaccinated against influenza, COVID, and other respiratory pathogens is less likely to carry and transmit those pathogens to the recipient. Keeping the people around you vaccinated is part of the protective environment.
When You Get Sick
And you will. Not a question of if.
Illness looks and behaves differently in an immunosuppressed recipient. Onset may be slower, but once an infection establishes, it runs harder and longer than it would in a healthy person. A cold that others clear in four or five days easily runs two weeks. The heaviest symptomatic period eventually passes, but the lingering tail—fatigue, residual congestion, general depletion—extends well past what the people around you experience. The immune system is clearing the infection, but it is doing so at a disadvantage, and the timeline reflects that.
More serious illness hits proportionally harder. The response that would normally contain a significant infection rapidly is operating at reduced capacity. This does not mean every illness becomes serious—most don’t—but it means the ceiling on how bad things can get is higher than it was pre-transplant.
The Standard Mild Illness Protocol
For a typical upper respiratory illness, the standard approach is supportive: rest, hydration, and Coricidin HBP—the formulation specifically for people who cannot take standard decongestants. The pseudoephedrine in regular cold preparations interacts with immunosuppressants and cardiovascular medications and is not appropriate for this population. Coricidin HBP addresses the symptoms without the problematic ingredient. The team is typically notified but does not necessarily intervene unless specific thresholds are crossed.
When to Call the Team
Fever above 100.4°F is the standard threshold: call immediately, do not wait to see if it resolves. Importantly, the fever response can sometimes be blunted under immunosuppression—the absence of high fever does not always indicate the absence of significant infection. Difficulty breathing, chest symptoms, any pattern suggesting more than a simple upper respiratory illness, and symptoms that worsen rather than plateau after 48—72 hours all warrant immediate contact with the transplant team. When in doubt, call. The team would rather hear from you at hour 24 than at hour 72.
When It Escalates
Active viral disease—CMV viremia, serious EBV reactivation, or other identified pathogens at significant levels—may require hospitalization for IV antiviral therapy. The oral prophylactics are maintenance tools; active disease sometimes requires IV-level intervention. This is not a common occurrence for most recipients managing a stable course, but it is part of the landscape worth understanding before it happens.
The Blood Work That Watches All of This
The post-transplant surveillance panel is not routine bloodwork. It is an active monitoring system tracking multiple dimensions of the transplant reality simultaneously. Understanding what it is measuring and why makes the cadence of draws and clinic visits comprehensible rather than arbitrary.
Trough levels—tacrolimus and sirolimus are drawn at the trough, immediately before the next dose, to measure the minimum circulating concentration. This is what the team uses to calibrate dosing. Too high: over-suppression, with increased infection and malignancy risk. Too low: under-suppression, with rejection risk. The target is a narrow band that moves over time as the protocol evolves and the graft stabilizes.
CBC with differential—the complete blood count and differential white cell breakdown tell the team whether the immune system is suppressed to target, over-suppressed (low total white count or neutropenia), or showing signs of mounting a response to something (elevated white count or specific cell line changes). Neutropenia—too-low neutrophil count—is a specific concern that can require protocol adjustments.
CMV and EBV PCR—quantitative viral load surveillance for the two most clinically significant viruses in this population. Not detected is the target for both. A detectable signal at low levels triggers closer monitoring. A rising signal triggers intervention. My own May 2026 EBV result—first detectable signal at <1.54 Log10 IU/mL and <35 IU/mL, flagged abnormal—is exactly this situation: something appearing where it wasn’t before, now being watched carefully.
TTV (Torque Teno Virus)—an emerging surveillance marker worth understanding, with the caveat that it is not yet a definitive standalone decision tool at most centers. TTV is a ubiquitous, generally harmless virus that a healthy immune system keeps suppressed. Higher TTV levels correlate with over-immunosuppression; lower or undetectable levels suggest the immune system is more active than intended. My November 2025 result was not detected; my May 2026 result registered at 1.02E+04 copies/mL—low abnormal, below the 1.00E+06 floor of the normal range. The juxtaposition with the first EBV signal appearing simultaneously is clinically interesting: TTV suggesting the immune system may be more active than targeted, while low-level EBV appearing suggests suppression is still sufficient to allow some viral reactivation. Two readings pointing in slightly different directions—precisely the kind of competing signal that makes post-transplant monitoring an ongoing calibration rather than a checkbox exercise.
DSA (Donor-Specific Antibodies)—the antibody-mediated rejection screen, checking for HLA antibodies directed specifically against the donor organ. My panel has been consistently negative across every draw from transplant through May 2026. Sustained DSA negativity is one of the most reassuring data points in the ongoing surveillance picture.
Prospera (donor-derived cell-free DNA)—the frontline noninvasive rejection screen. Think of it as a smoke detector: it doesn’t tell you why cells are shedding DNA into the bloodstream, but it tells you they are—which is the earliest detectable signal of graft cell death before clinical symptoms appear. A rising dd-cfDNA result prompts further investigation; a stable, low result is reassurance that the graft is not under active attack.
The Cancer Risk: What Discharge Paperwork Doesn’t Adequately Cover
Chronic immunosuppression impairs the immune system’s cancer surveillance function. Under normal circumstances, the immune system identifies and destroys aberrant cells before they establish as tumors—a continuous background process most people are never aware of. Under sustained suppression, that surveillance is compromised. Cells that would normally be caught and cleared early get more time to proliferate and establish.
This is one of the most significant long-term risks of life after transplant, and it is frequently underemphasized at discharge—not because the teams are unaware of it, but because patients in the immediate post-surgical period are managing enough information already. It deserves more prominent and earlier discussion than it typically receives.
Skin Cancer: The Primary Risk
Heart transplant recipients face a dramatically elevated skin cancer risk—higher, specifically, than other solid organ transplant recipients, attributed to the heavier immunosuppression required to maintain cardiac graft survival. A 10-year retrospective cohort study of 6,271 heart transplants at 32 US centers found that squamous cell carcinoma incidence increased 4- to 30-fold compared to the age and gender equivalent general population.
The nature of the risk is distinct from the general population in a specific and important way. In immune-competent adults, basal cell carcinoma is far more common than squamous cell carcinoma—roughly a 4:1 ratio. In transplant recipients, that ratio flips to 5:1 in favor of SCC. The rarer, more aggressive cancer becomes the more common one. Cumulative incidence of any skin cancer reaches 20% at five years, 37% at ten years, and 46% at fifteen years post-transplant.
The mechanism is straightforward: UV radiation causes DNA damage in skin cells. Under normal immune surveillance, those damaged cells are identified and cleared. Under immunosuppression, they accumulate. Sun exposure—which most people treat as a casual environmental background—becomes an active, ongoing, manageable risk factor.
The practical response: SPF 50+ daily, regardless of cloud cover, season, or planned duration outdoors. UPF-rated clothing for extended outdoor exposure. And a dermatologist as a permanent member of the care team, with annual full-body skin surveillance. New or changing lesions—anything that grows, bleeds, changes color, or doesn’t heal normally—warrant immediate contact with the team rather than waiting for the next scheduled visit.
Beyond Skin: The Broader Malignancy Picture
Skin cancer is the most prevalent post-transplant malignancy, but not the only one worth understanding.Overall de novo malignancy risk in cardiac transplant recipients runs 2- to 4-fold above the general population, with an approximately 20% cumulative incidence at ten years of chronic immunosuppression. Cardiac recipients face a higher overall malignancy burden than renal transplant recipients—visceral cancers approximately 6-fold more prevalent, lymphoma risk approximately 4-fold higher—attributed to the heavier suppression load that cardiac graft maintenance requires.
PTLD: Post-Transplant Lymphoproliferative Disorder
PTLD is the most common non-skin malignancy in solid organ transplant recipients. It is driven by Epstein-Barr virus reactivation under immunosuppression—the virus that causes mononucleosis, kept latent in most adults by intact immune surveillance, and given an opportunity to drive abnormal B-cell proliferation when that surveillance is compromised. Median time from transplant to PTLD is approximately 8.5 years, making this a long-game risk rather than an immediate concern. The EBV PCR surveillance in the standard monitoring panel exists precisely to catch early reactivation signals before they progress.
The Sirolimus Effect
There is a meaningful silver lining that connects directly to the CAV management discussion elsewhere in this series. Sirolimus-based immunosuppression has demonstrated reduced risk of overall post-transplant malignancies including PTLD, related to its inhibitory effects on the mTOR pathway—the same pathway involved in tumor cell growth and proliferation. Recipients on sirolimus-based regimens appear to have lower malignancy rates than those on calcineurin inhibitor-only protocols. For recipients already on sirolimus for CAV management, this represents the drug doing meaningful double duty.
Masks, Gloves, and the Hierarchy of Protection
The goal of daily infection prevention is not hermetic sealing. It is informed, calibrated risk reduction—understanding the actual risk of a given environment and making a proportionate response to it. The restrictions of Phase One are not the appropriate framework for Phase Two, and treating them as equivalent produces both unnecessary restriction and, eventually, fatigue that undermines the precautions that actually matter.
Masks
During Phase One, indoor masking is the correct default. During cold, flu, and COVID season—roughly October through April in the Northern Hemisphere—indoor masking remains appropriate regardless of suppression phase, because the viral load in the environment is genuinely higher and the immune system’s ability to handle respiratory pathogens is genuinely reduced.
In the warm months, the calculus loosens. Viral circulation is lower. Ventilation is often better. The outdoor environment carries minimal transmission risk for most respiratory pathogens. The read becomes environmental: crowd density, airflow, season, and current suppression level all factor into whether masking is warranted in a given situation.
A practical example from my own recent experience: picking up an order at a local hardware store on a May morning. Front door open. Two other people in the building. I went in without a mask. That is not recklessness. That is what informed judgment looks like in practice—reading the specific environment against the current risk profile and making a proportionate decision. The same judgment that would have me masked without question in a crowded urgent care waiting room in January.
Gloves: The False Confidence Problem
Gloves carry a specific and underappreciated risk: false confidence. A recipient wearing gloves who doesn’t recognize the cross-contamination problem may introduce more pathogen transfer, not less, because the gloves create a sense of protection that reduces the behavioral vigilance that actually does the work.
Gloves pick up everything hands pick up. Every surface touched with a contaminated glove transfers that contamination to the next surface. A recipient who touches a shopping cart, then their phone, then their face while wearing gloves has not protected themselves—they have simply added an intermediary layer that they are not treating as contaminated. Add improper removal technique—touching the outside of the glove during doffing—and the protection is entirely illusory.
When gloves genuinely help: handling medications (some immunosuppressants carry teratogenic risk for others in the household), cleaning, and high-contact surface work in demonstrably high-risk environments. The Things You Need has specific nitrile glove recommendations for this population.
Hand Hygiene: The Intervention That Actually Works
Hand hygiene is consistently the most effective single infection prevention intervention available, and it is consistently undervalued relative to more visible measures like gloves and masks. Washing hands properly—twenty seconds, full coverage including between fingers and under nails—before eating, after any public contact, and after touching shared surfaces removes the actual transmission vector rather than creating an intervening layer. Keeping hands away from the face—particularly eyes, nose, and mouth, which are the primary entry points for respiratory pathogens—is the behavioral complement to hand washing.
For situations where soap and water aren’t immediately available, PDI Sani-Hands wipes kept in the car provide reliable sanitation. The full suite of recommended hygiene and sanitation products for transplant recipients is at The Things You Need.
Environmental Hazards
Several environmental risks are elevated for immunosuppressed recipients in ways that are not intuitively obvious and are rarely explained at discharge. These are manageable risks, not prohibitions against engaging with the world—but they require awareness and specific precautions that immune-competent people don’t need to think about.
Soil and gardening—Soil harbors fungal spores—Aspergillus, Histoplasma, Cryptococcus—that a healthy immune system encounters and clears without incident but that can cause serious invasive infection in the immunosuppressed. The risk is not that dirt is inherently dangerous; it is that specific organisms present in soil, particularly when aerosolized by disturbing dry soil or compost, can be inhaled and establish in a lung that cannot clear them efficiently. Gardening is possible, but requires gloves without exception and a mask when working with dry or disturbed soil.
Cat litter—toxoplasmosis—Toxoplasma gondii is shed in cat feces. In immune-competent adults, toxoplasmosis causes mild or no symptoms. In the immunosuppressed, it can cause severe neurological disease. Do not handle cat litter. This is not a temporary restriction and it is not negotiable.
Rodent droppings and urine—hantavirus—Hantavirus is transmitted through contact with or inhalation of aerosolized particles from rodent droppings, urine, or nesting material. Avoid any environment with visible evidence of rodent activity. If remediation is necessary, do not perform it yourself.
Birds—fungal risk—Bird droppings are a vector for Cryptococcus neoformans and Histoplasma capsulatum—fungal pathogens capable of causing serious systemic infection in immunosuppressed recipients. The restriction around birds is not about the birds themselves but about the environmental fungal load associated with droppings, roosting sites, coops, and aviaries.
Children—Children are efficient vectors for every respiratory virus in active circulation, managing these infections with their developing immune systems while broadcasting them generously to the environment around them. The healthy child is not the specific risk; the sick child is.
Toilet flushing—aerosolization—Every flush generates a fine aerosol that travels well beyond the bowl—studies have documented bacterial and viral particles landing on surfaces up to six feet away, including toothbrushes left on the counter. Close the lid before flushing. Keep toothbrushes in a closed cabinet or at a meaningful distance from the toilet. This is not a post-transplant peculiarity; it is basic physics that most people simply ignore because the immune-competent body handles the exposure without consequence.
Natural water—rivers, lakes, oceans—Open water bodies carry a range of pathogens that represent minimal risk to a healthy swimmer and a real risk to the immunosuppressed: Cryptosporidium, Giardia, Naegleria fowleri in warm freshwater, various Vibrio species in marine environments, and cyanobacterial toxins in algae-blooming lakes. Swimming is not categorically prohibited, but swallowing water should be actively avoided, any open wound or skin break is a genuine concern near natural water, and heavily algae-bloomed water warrants avoidance entirely. The ocean is generally lower-risk than freshwater lakes and rivers, but it is not pathogen-free.
The Calculus Is Always Changing
The goal of post-transplant life is not the elimination of all risk. It is learning which risks matter, which ones change over time, and which ones become permanent features of the landscape—and making informed decisions within that understanding rather than either reckless ones or unnecessarily restrictive ones that cost quality of life without reducing meaningful risk.
Some of what the first year requires is temporary scaffolding. The prophylactic medications. The maximum-caution masking. The avoidance of environments that Phase Two will eventually allow. Those come down as the graft stabilizes and suppression is reduced, and they should. Some of it doesn’t go back. The sun protection. The annual dermatology surveillance. The EBV monitoring. The awareness of environmental fungal risks. These are permanent additions to the operating system—not inconveniences to be eventually discarded, but recalibrations of how a person with a transplanted heart relates to the physical world.
Understanding which category any given restriction falls into—temporary scaffolding or permanent recalibration—is the practical work of post-transplant life. The restrictions appropriate to month three are not the restrictions appropriate to month eighteen. The biology explains the difference. The surveillance data confirms it in real time.
The social and emotional reality of living within these constraints—what it costs, what it takes from ordinary life, and where it eventually settles—is the subject of the companion piece to this one.
Key Terms
Full definitions at the One More Beat Glossary: onemorebeat.com/glossary/
Calcineurin Inhibitor—A class of immunosuppressant that blocks T-cell activation. Tacrolimus (Prograf/Envarsus) is the most commonly used agent in heart transplant recipients.
CMV (Cytomegalovirus)—A common herpesvirus that can cause serious disease in immunosuppressed recipients. CMV-negative recipients receiving a CMV-positive donor organ (D+/R-) face the highest primary infection risk.
dd-cfDNA (Donor-Derived Cell-Free DNA)—DNA fragments shed by graft cells into the bloodstream, measurable by the Prospera test. Elevated levels signal graft cell death and possible rejection.
DSA (Donor-Specific Antibodies)—Antibodies directed against HLA antigens of the donor organ. Persistent DSA positivity is associated with antibody-mediated rejection.
EBV (Epstein-Barr Virus)—The virus responsible for mononucleosis, kept latent in most adults by intact immune surveillance. Reactivation under immunosuppression is the primary driver of PTLD.
Neutropenia—Abnormally low neutrophil count. A specific risk with some immunosuppressive agents that can require protocol adjustment.
PCP (Pneumocystis jirovecii Pneumonia)—A fungal pneumonia rarely seen in immune-competent adults that can be catastrophic in the immunosuppressed. Prevented by Bactrim prophylaxis.
PTLD (Post-Transplant Lymphoproliferative Disorder)—The most common non-skin malignancy in solid organ transplant recipients. Driven by EBV reactivation under immunosuppression.
Trough Level—The minimum blood concentration of a medication, measured immediately before the next dose. Used to calibrate immunosuppressant dosing.
TTV (Torque Teno Virus)—An emerging biomarker of overall immune function. Higher levels suggest over-immunosuppression; lower or absent levels suggest a more active immune state than targeted. Not yet a definitive standalone clinical tool.
Further Reading
One More Beat Glossary: onemorebeat.com/glossary/
The Things You Need: onemorebeat.com/the-things-you-need/
Skin Cancer After Heart Transplantation—Systematic Review (2025): PubMed Central
Increased Incidence and Mortality of Skin Cancers After Cardiac Transplant: American Journal of Transplantation
Temporal Trends of De Novo Malignancy After Heart Transplantation: Journal of the American College of CardiologyPTLD After Cardiac Transplantation: Frontiers in Cardiovascular Medicine
Discover more from One More Beat
Subscribe to get the latest posts sent to your email.