What We Take and Why: Immunosuppression
The transplanted heart is living tissue carrying someone else’s genetic signature. The immune system was built to recognize anything carrying a genetic signature that isn’t yours—and to treat it as a threat. That is not a malfunction. That is the immune system doing exactly what it was designed to do.
Immunosuppression exists to prevent that response from destroying the organ. It is not a temporary course of treatment while the body adjusts. It is an ongoing requirement for the life of the transplant. Without it, the immune system would eventually win.
The intensity of that suppression, however, is not fixed. In the days and weeks immediately following surgery, when rejection risk is highest, suppression is deliberately aggressive. As stability is established and the risk profile changes over months and years, doses come down and some medications are tapered off entirely. And when a recipient becomes seriously ill—a significant infection, for example—the team may reduce immunosuppression temporarily to give the immune system room to fight, accepting a degree of rejection risk to manage the immediate threat. The medications are a managed variable, not a permanent fixed setting.
The goal throughout is balance: enough suppression to prevent rejection, not so much that infection and other complications become unmanageable. Finding and maintaining that balance is what the monitoring, the dose adjustments, and the bloodwork are all doing.
(For information on other meds we commonly take, see What We Take and Why: Supporting Cast.)
The First Days: Induction
The period immediately following transplant has its own distinct immunosuppression strategy, separate from the long-term maintenance regimen. Depending on the recipient’s risk profile, several agents may work together in those first days to hit the immune system hard and fast during the window of highest rejection risk.
High-dose corticosteroids—typically intravenous methylprednisolone in the operating room, transitioning to high-dose oral prednisone—provide broad-spectrum immune suppression across multiple pathways simultaneously. The dose in this window is substantially higher than anything a recipient will take long-term, which is why early post-transplant side effects are so pronounced.
Basiliximab (Simulect) is a monoclonal antibody that targets the IL-2 receptor on T-cells—blocking the signal that triggers T-cell proliferation. It is given as two doses, typically on the day of transplant and four days later, then it is done. Most recipients receive it only at induction.
Antithymocyte globulin (ATG, Thymoglobulin) is more aggressive: rather than blocking a signal, it depletes T-cells directly. Used when the team wants deeper induction—typically in recipients at higher immunological risk—it is administered over several days and then discontinued. Like basiliximab, it does not reappear in the maintenance regimen.
These three are not redundant. They are complementary, each working at a different point in the immune response to provide overlapping coverage during the most critical period. Recipients who remember receiving medications in the hospital that then disappeared are usually remembering basiliximab or ATG. Their absence afterward is normal and expected.
The pronounced exhaustion and immune suppression of early recovery is, in significant part, pharmacological and intentional. The team was doing something deliberate.
The Maintenance Regimen: Three Tiers
Once the induction period passes, the long-term maintenance regimen takes over. Most heart transplant recipients are managed on a triple-therapy protocol drawn from three distinct drug classes, each targeting a different part of the immune response.
Calcineurin inhibitors block T-cell activation at the source—preventing the immune system from initiating the attack.
Antiproliferatives prevent activated immune cells from multiplying—containing the response if activation begins.
Corticosteroids provide broad-spectrum suppression across multiple immune pathways—the same class used in induction, now at substantially lower doses.
A fourth class—mTOR inhibitors—is not typically part of the initial maintenance regimen but enters the picture in specific clinical circumstances, discussed below.
Why Combination Therapy
The immune system is not a single pathway. It is a network of overlapping signals and responses, each capable of initiating or amplifying an attack on foreign tissue. Using smaller amounts of several medications that act at different points in that network is generally more effective—and often safer—than relying on very high doses of a single drug. Each medication can be dosed lower than it would need to be if it were working alone, which reduces the toxicity burden of any one agent while maintaining overall suppression.
This is why a recipient takes multiple pills. It is not redundancy. It is strategy.
Calcineurin Inhibitors
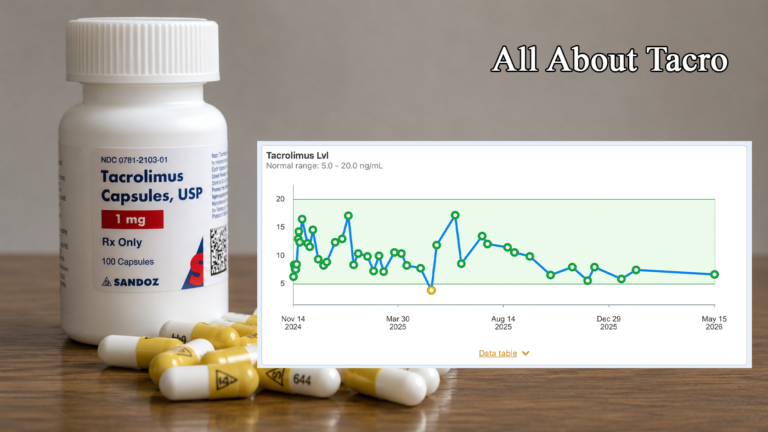
Tacrolimus (Prograf, Envarsus XR) is the primary calcineurin inhibitor for most heart transplant recipients today. It blocks the calcineurin pathway, preventing T-cells from receiving the chemical signal that triggers activation and proliferation. Without that signal, the primary attack cells of the immune system remain quiet.
Tacrolimus is monitored via trough levels—blood drawn immediately before a dose, capturing the lowest point in the medication cycle. The therapeutic window is narrow: levels too low leave the organ inadequately protected; levels too high accumulate toxicity over time. Target ranges are individualized and shift over time post-transplant—the number the team is aiming for in month one is not the same number they are aiming for in year three. That narrow window is why the bloodwork matters so much and why consistency of dosing, timing, and formulation is not optional.
Envarsus XR is an extended-release formulation of tacrolimus designed for once-daily dosing. It delivers the same active medication through a different release mechanism and is not directly interchangeable milligram-for-milligram with immediate-release Prograf. Recipients on one formulation should not switch without team guidance. Dose conversions between formulations are well-established, but they are not one-to-one. For a full treatment of tacrolimus—mechanism, monitoring, interactions, and long-term management—see All About Tacrolimus.
Side effects in plain language: tremors (common, particularly early, often improve as doses are adjusted downward), insomnia, headaches, elevated blood sugar, magnesium depletion, hair loss (alopecia), and nephrotoxicity at higher levels over time. Not every recipient experiences all of these, and severity varies considerably.
Cyclosporine (Neoral, Sandimmune, Gengraf) is the older calcineurin inhibitor—the drug that made transplant medicine viable at scale when it was approved in 1983, before tacrolimus largely displaced it based on lower acute rejection rates. It is still used in some recipients, particularly those who do not tolerate tacrolimus well.
The side effect profiles differ in clinically meaningful ways. Cyclosporine has a more pronounced effect on blood pressure and cholesterol; tacrolimus is more diabetogenic. Cyclosporine is also associated with hirsutism—unwanted hair growth—which is one of the reasons many recipients and clinicians have preferred tacrolimus where both are tolerated. Neither is universally superior; the choice depends on the individual recipient’s clinical picture.
Both tacrolimus and cyclosporine have narrow therapeutic windows, which means consistency of formulation matters. Generic immediate-release versions of both are widely used and generally perform well. If a pharmacy changes suppliers on either medication, note it. Most of the time nothing changes. Occasionally it becomes a useful data point when a trough level moves unexpectedly. Mention it to the team.
Antiproliferatives
Mycophenolate mofetil (CellCept) and mycophenolate sodium (Myfortic) are the standard antiproliferative agents in the maintenance regimen. They inhibit an enzyme—inosine monophosphate dehydrogenase—that lymphocytes require to synthesize DNA and proliferate. Where the calcineurin inhibitor prevents T-cell activation, mycophenolate prevents activated immune cells from multiplying. The two work at different points in the same cascade, which is why using both is more effective than either alone.
GI side effects are common, particularly early: nausea, loose stool, cramping. Often manageable with dose timing or formulation adjustments—Myfortic’s enteric coating was developed specifically to reduce GI burden. Mycophenolate can also suppress bone marrow function, leading to reductions in white blood cell counts. When a recipient hears “we’re reducing your CellCept because your white count is low,” that is the mechanism at work. Mycophenolate is also known to cause serious fetal harm and is generally avoided during pregnancy; this is discussed further in the azathioprine section below.
Mycophenolate has significant interactions with magnesium-containing antacids and with certain foods and supplements. For the full interaction picture, see What to Avoid and Why.
Azathioprine (Imuran) is the older antiproliferative, used before mycophenolate became standard. Less common in newly transplanted recipients today, it is still present in some longer-term recipients who were established on it before mycophenolate became standard. It has a different toxicity profile—more bone marrow suppression, less GI burden. One circumstance where it is still preferred: recipients who are or may become pregnant. Given mycophenolate’s teratogenicity, azathioprine carries meaningfully lower fetal risk and may be the appropriate choice in that context.
Corticosteroids
Prednisone is the third element of the standard triple therapy, and the one whose role changes most dramatically over time. It starts at high doses immediately post-transplant for broad-spectrum immune suppression, then tapers progressively over months as the calcineurin inhibitor and antiproliferative establish stable coverage.
Of all the transplant medications, prednisone is often the one recipients feel most directly. Tacrolimus may show up in bloodwork; prednisone frequently shows up in the mirror, on the scale, and in the way a person feels day to day. Weight gain, fluid retention, elevated blood sugar, mood effects, insomnia, and bone density loss are all documented at higher doses. Most of these improve significantly as the dose comes down—what felt like a heavy blanket at 20 or 30mg often feels like a light shirt at 5mg or less.
How aggressively prednisone is tapered varies substantially by transplant center. Some programs pursue steroid withdrawal—getting recipients off prednisone entirely—within the first year. Others maintain recipients on low-dose prednisone indefinitely. Neither approach is universally correct; the decision reflects the center’s clinical philosophy, the recipient’s rejection history, and individual risk factors.
The full story of prednisone—how it is used in transplant versus general medicine, the induction dose, the taper arc, and what long-term management looks like—will be covered in All About Prednisone.
mTOR Inhibitors
Sirolimus (Rapamune) and everolimus (Zortress) belong to a distinct drug class that targets a different pathway from calcineurin inhibitors. Rather than blocking T-cell activation, mTOR inhibitors interfere with the downstream signaling that drives cell proliferation and growth.
These are not typically part of the starting maintenance regimen, for a specific reason: mTOR inhibitors impair wound healing. In the immediate post-transplant period, when surgical sites are still healing and the body is recovering from major intervention, introducing an agent with that effect is inadvisable. The team will not reach for sirolimus or everolimus until that window has safely passed.
They appear in the clinical picture in two main scenarios. The first is nephroprotection: when tacrolimus is causing significant kidney toxicity over time, introducing or transitioning to an mTOR-based regimen can reduce the calcineurin inhibitor burden and slow the progression of renal damage. The second is CAV management: mTOR inhibitors have demonstrated antiproliferative effects on the coronary vasculature, making them relevant in the management of cardiac allograft vasculopathy.
The medication beginning with S that comes up frequently in transplant groups is almost certainly sirolimus. It is a legitimate drug used in real clinical circumstances. It is not an alternative a recipient elects to start on their own, and it is not without its own side effect profile: elevated lipids, mouth sores, impaired wound healing, and in some recipients, interstitial pneumonitis—a rare inflammation of the lung tissue. The team reaches for it when the clinical picture calls for it.
Why the Monitoring Isn’t Optional
These medications work within narrow margins. Levels too low and the immune system has room to mount a rejection response. Levels too high and toxicity accumulates—kidney damage, infection risk, and the longer-term complications that chronic immunosuppression creates. The bloodwork is not administrative. It is the instrument by which the team keeps the regimen in the zone where it is doing its job without doing damage.
The regimen also changes over time. Doses adjust as the body and the organ reach a new equilibrium. A medication may be tapered, added, or swapped as the clinical picture evolves. That is expected and normal, not a sign that something has gone wrong. No two recipients have exactly the same regimen. Differences in age, rejection history, kidney function, infection risk, side effects, and center practices all influence what a particular recipient ultimately takes. The team managing these adjustments has a complete picture of the recipient’s history and risk profile that no article can replicate.
For a deeper look at what the monitoring numbers mean and what moves them, see The Blood Is the Life.
A Note on Brand Names and Generics
Most of the medications discussed here are available in both brand-name and generic formulations. Generic equivalents are widely used, generally well-regulated, and perform well for most recipients. The exception worth noting is the calcineurin inhibitors—tacrolimus and cyclosporine—where the narrow therapeutic window means that even small differences between formulations can shift trough levels in ways that become clinically relevant.
Many transplant centers prefer that recipients on calcineurin inhibitors remain on the same manufacturer’s formulation whenever possible. If a pharmacy changes suppliers—which happens without notice—make a note of it and mention it at the next clinic visit if levels move unexpectedly. It is not a reason for alarm. It is a useful data point.
For More
This piece covers the landscape. For the deeper treatment of individual medications: All About Tacrolimus covers mechanism, monitoring, interactions, and long-term management in full. All About Prednisone covers the arc from induction dose to long-term management. For the complete picture of what interacts with these medications—foods, supplements, and over-the-counter drugs—see What to Avoid and Why. For the bloodwork and monitoring numbers in context, see The Blood Is the Life.
Discover more from One More Beat
Subscribe to get the latest posts sent to your email.